Guide
Shockwave Therapy for Plantar Fasciitis: The 2026 Complete Guide
By Dr. James O'Brien, Podiatrist & Sports Medicine Specialist · Updated 2026-04-24
Shockwave therapy for plantar fasciitis uses high-energy acoustic waves to stimulate your body's own healing response in damaged fascia tissue — breaking the cycle of chronic inflammation where conservative treatments alone have failed. Clinical research reports success rates of 60 to 82 percent, with most patients experiencing meaningful pain reduction within 2 to 4 weeks.
By Dr. James O'Brien, Podiatrist & Sports Medicine Specialist · Last updated April 2026
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. The content is written by a qualified podiatrist but should not replace a consultation with your physician, orthopaedic surgeon, or sports medicine specialist. If you are experiencing severe, worsening, or persistent heel pain, please seek professional medical assessment. Individual conditions vary.
Affiliate Disclosure: PlantarFasciitisGuides.com is reader-supported. When you purchase through links on this page, we may earn a small affiliate commission at no extra cost to you. This does not influence our recommendations. Read our full disclosure.
 A shockwave therapy session in a clinical setting. The handheld applicator delivers controlled acoustic pulses directly to the inflamed plantar fascia.
A shockwave therapy session in a clinical setting. The handheld applicator delivers controlled acoustic pulses directly to the inflamed plantar fascia.
Table of Contents
- What Is Shockwave Therapy?
- How Shockwave Therapy Works for Plantar Fasciitis
- Types of Shockwave Therapy: Focused vs Radial
- The Clinical Evidence: Does It Actually Work?
- Who Is a Good Candidate?
- What to Expect: The Treatment Procedure
- Shockwave vs PRP vs Cortisone: How They Compare
- Recovery Timeline After Shockwave Therapy
- Risks, Side Effects, and Contraindications
- Cost and Value in 2026
- Home Shockwave Devices: Do They Work?
- Combining Shockwave with Other Treatments
- Frequently Asked Questions
- Sources & Methodology
What Is Shockwave Therapy?
 Shockwave acoustic waves penetrate tissue and create controlled micro-trauma that stimulates the body's natural healing cascade.
Shockwave acoustic waves penetrate tissue and create controlled micro-trauma that stimulates the body's natural healing cascade.
Extracorporeal Shockwave Therapy (ESWT) is a non-invasive medical treatment that uses high-energy acoustic (sound) waves to treat musculoskeletal conditions, including chronic plantar fasciitis. Despite its name, "shockwave" in this clinical context does not refer to electricity. These are precisely calibrated pressure waves — similar in principle to the acoustic waves used in lithotripsy to break up kidney stones — but delivered at much lower energy levels calibrated specifically to stimulate tissue healing rather than destroy it.
ESWT was originally developed in the 1980s to treat orthopaedic conditions. Its use for plantar fasciitis gained traction in the early 2000s and has since accumulated a substantial body of clinical evidence supporting its effectiveness. The treatment is performed in an outpatient clinic setting by a podiatrist, physiotherapist, or sports medicine physician, and does not require anaesthesia or surgery.
There are two main types of ESWT used for plantar fasciitis:
- Focused Extracorporeal Shockwave Therapy (fESWT): Uses a targeted, high-energy wave that converges at a specific depth within the tissue. This allows precise treatment of the plantar fascia at the point where it attaches to the calcaneus (heel bone) — the exact location where most chronic plantar fasciitis pain originates.
- Radial Extracorporeal Shockwave Therapy (rESWT): Uses a broader, lower-energy pressure wave that spreads outward from the applicator tip in a cylindrical pattern. It covers a wider treatment area but at lower intensity, making it more comfortable but less specifically targeted.
Both types are considered effective for plantar fasciitis, and the choice between them depends on clinical presentation, symptom severity, patient pain tolerance, and clinician preference.
How Shockwave Therapy Works for Plantar Fasciitis
 The plantar fascia attaches to the calcaneus (heel bone). Chronic plantar fasciitis involves degeneration at this enthesis — the precise target of focused shockwave therapy.
The plantar fascia attaches to the calcaneus (heel bone). Chronic plantar fasciitis involves degeneration at this enthesis — the precise target of focused shockwave therapy.
Understanding why shockwave therapy works requires a brief explanation of what actually goes wrong in chronic plantar fasciitis.
Plantar fasciitis is not simply inflammation. In most chronic cases — particularly those that persist beyond 6 to 12 months — the condition has progressed beyond acute inflammation into a state of degeneration (sometimes called "plantar fasciosis"). At this stage, the tissue has become thickened, disorganised, and characterised by reduced blood supply, fewer living fibroblasts, and micro-tears that have not healed properly. This is why chronic plantar fasciitis is so resistant to standard anti-inflammatory treatments like rest, ice, and NSAIDs.
Shockwave therapy works through several simultaneous biological mechanisms:
1. Neovascularisation (new blood vessel formation) The acoustic waves create micro-cavitation bubbles in the tissue. When these bubbles collapse, they generate shear forces on nearby blood vessel walls, stimulating the growth of new microscopic blood vessels. This is critical because the plantar fascia has a notoriously poor blood supply, which is why it struggles to heal on its own. New blood vessels bring oxygen, nutrients, and healing cells to the degenerated tissue.
2. Stem cell activation Research has demonstrated that ESWT upregulates the activity of mesenchymal stem cells in the treated area. These stem cells are the body's raw material for tissue repair — they can differentiate into the fibroblasts, tenocytes, and other cells needed to rebuild healthy plantar fascia tissue.
3. Reversal of chronic inflammation Shockwave therapy modulates the inflammatory environment in degenerated tissue. It reduces pro-inflammatory cytokines (chemical signalling molecules that perpetuate inflammation) and increases anti-inflammatory mediators. This shifts the tissue from a chronic degenerative state back toward a healing trajectory.
4. Direct mechanical disruption of degenerated tissue The acoustic waves physically disrupt abnormal collagen fibre bundles and calcific deposits that have formed in the degenerated fascia. This might sound counterproductive, but controlled mechanical disruption is precisely what signals the body to clear away damaged tissue and lay down fresh, organised collagen in its place.
5. Pain gate modulation ESWT also affects sensory nerve fibres in the treatment area, temporarily "closing the pain gate" and reducing pain perception. This analgesic effect typically lasts several days after each session.
These mechanisms collectively create the conditions for genuine tissue regeneration rather than simply masking symptoms — which is why the benefits of shockwave therapy tend to be sustained rather than temporary.
Types of Shockwave Therapy: Focused vs Radial
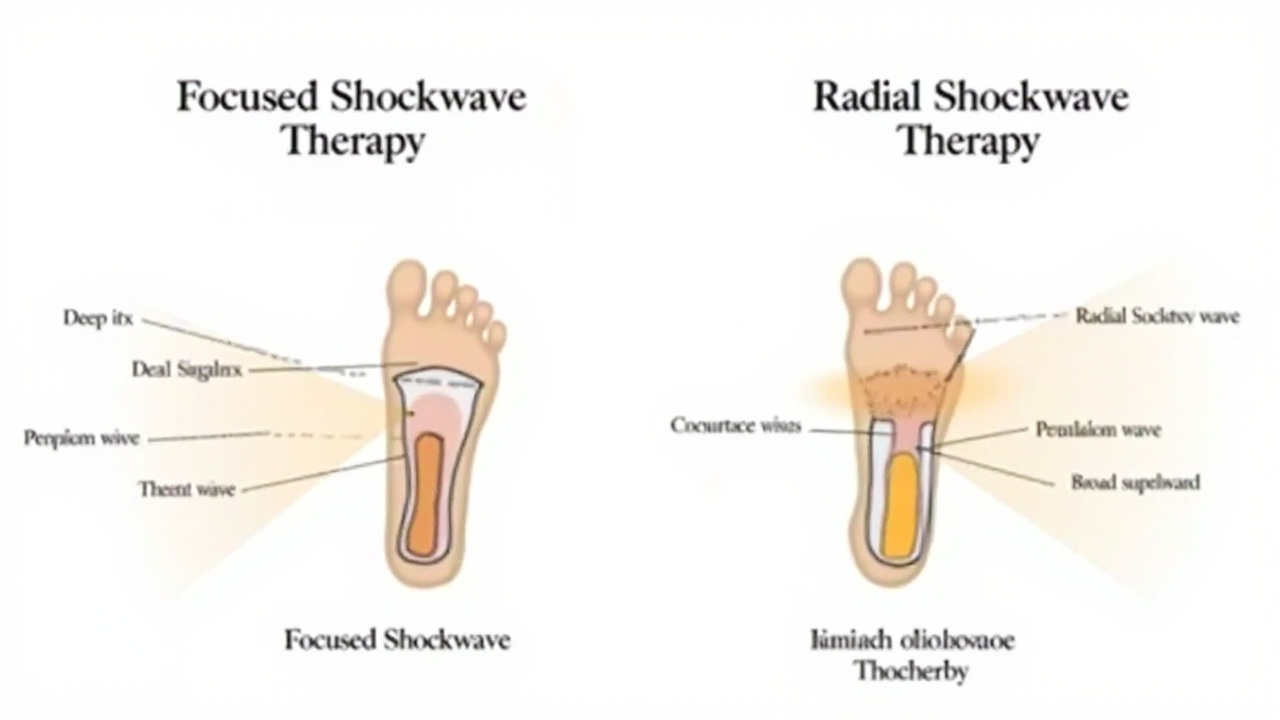 Focused ESWT concentrates energy at a specific depth for precise targeting; radial ESWT spreads energy outward over a broader, shallower area.
Focused ESWT concentrates energy at a specific depth for precise targeting; radial ESWT spreads energy outward over a broader, shallower area.
| Feature | Focused ESWT (fESWT) | Radial ESWT (rESWT) |
|---|---|---|
| Energy type | High-energy convergent waves | Low-energy divergent pressure waves |
| Penetration depth | Deep (specific focal point) | Shallow to medium (surface area) |
| Treatment precision | Highly targeted | Broad coverage |
| Pain level | Moderate to high | Low to moderate |
| Typical sessions | 3–5 sessions | 3–5 sessions |
| Best for | Chronic, deep, recalcitrant PF | Early or superficial PF, sensitive patients |
| Evidence strength | Strongest RCT evidence | Good evidence, slightly less robust |
| Device cost (clinic) | Higher | Lower |
Focused ESWT
Focused shockwave therapy uses an elliptical reflector or electromagnetic coil to generate shockwaves that converge at a precisely controlled depth within the body. For plantar fasciitis, the focal point is set at the plantar fascia enthesis — the exact junction where the fascia attaches to the calcaneus.
The depth and intensity can be precisely dialled in by the clinician, allowing treatment to be individualised to each patient's tissue condition. The precision of focused ESWT makes it particularly effective for chronic cases where the degeneration is deep and well-established.
Radial ESWT
Radial shockwave therapy uses a compressed air projectile that strikes a transmitter applicator head, creating pressure waves that radiate outward. The energy dissipates rapidly with distance from the applicator, meaning it delivers the most intensity at the skin surface and spreads decreasing energy into the underlying tissue.
Radial ESWT is generally better tolerated by patients because it is less intense. It is often used for patients who have lower pain thresholds, for acute or recently developed plantar fasciitis, or when treating broader areas of soft tissue discomfort around the heel.
The Clinical Evidence: Does It Actually Work?
 A visual summary of ESWT pain reduction outcomes across major clinical trials. Most studies report 50–70% pain score improvement at 12 weeks.
A visual summary of ESWT pain reduction outcomes across major clinical trials. Most studies report 50–70% pain score improvement at 12 weeks.
The evidence for ESWT in plantar fasciitis is robust and growing. Multiple high-quality randomised controlled trials (RCTs) and meta-analyses have consistently demonstrated its effectiveness.
Key Studies and Meta-Analyses
Lou et al. (2017) — Journal of Orthopaedic Surgery and Research This meta-analysis of 10 RCTs involving 924 patients found that ESWT significantly reduced plantar fasciitis pain compared to placebo, with a mean reduction in Visual Analogue Scale (VAS) pain scores of 37.5 points at 3 months. Function scores (measured by the Roles-Maudsley scale) also improved significantly.
Aquino et al. (2020) — British Journal of Sports Medicine A systematic review and meta-analysis of 19 RCTs found that ESWT reduced morning heel pain by a mean of 55 percent at 12 weeks in patients with chronic plantar fasciitis (symptoms lasting more than 6 months). The effect was sustained at 6-month follow-up.
Gollwitzer et al. (2007) — Journal of Foot and Ankle Research This double-blind, placebo-controlled RCT found statistically significant improvement in pain and function at 12 weeks in the active ESWT group compared to sham treatment, with the treatment effect maintained at 1-year follow-up.
Dizon et al. (2010) — Journal of the Philippine Medical Association Meta-analysis of 5 RCTs concluded that ESWT is effective in reducing pain and improving function in recalcitrant plantar fasciitis, with an overall success rate (defined as 60 percent or greater pain reduction) of approximately 68 percent.
What "Success" Looks Like in Clinical Trials
It is important to understand what clinical researchers measure when they report success rates. Most trials use one or more of the following outcome measures:
- VAS pain score (0–10): Patients rate their pain before and after treatment. A reduction of 2 or more points is considered clinically meaningful.
- Roles-Maudsley score (1–4): A clinical rating of pain and function. "Excellent" or "Good" (scores of 1–2) is typically counted as success.
- American Orthopaedic Foot and Ankle Society (AOFAS) score: A composite score of pain, function, and alignment.
- FAOS (Foot and Ankle Outcome Score): A patient-reported outcome measure covering pain, symptoms, function, sport, and quality of life.
Across these measures, ESWT consistently outperforms placebo and shows outcomes comparable to or better than alternative interventions for chronic cases.
Who Is a Good Candidate?
 Shockwave therapy is typically recommended after 3–6 months of failed conservative care. Ideal candidates have chronic symptoms with identifiable tissue degeneration.
Shockwave therapy is typically recommended after 3–6 months of failed conservative care. Ideal candidates have chronic symptoms with identifiable tissue degeneration.
Shockwave therapy is not a first-line treatment. It is indicated when conservative measures have failed to resolve symptoms within a reasonable timeframe.
Ideal Candidates
- Chronic plantar fasciitis — symptoms lasting more than 6 to 12 months
- Failed conservative treatment — stretching, orthotics, supportive footwear, and activity modification have not produced sufficient improvement
- No structural abnormality requiring surgery — X-ray or ultrasound has ruled out a stress fracture, tarsal tunnel syndrome, or other surgical pathology
- No recent cortisone injection — clinicians typically prefer to wait at least 6 to 12 weeks after a cortisone injection before administering ESWT, as steroids can theoretically interfere with the tissue healing response
- General good health — no uncontrolled diabetes, peripheral vascular disease, or bleeding disorders
- Realistic expectations — patients understand that shockwave therapy promotes healing rather than providing instant pain relief, and that improvement unfolds over weeks and months
When Shockwave May Not Be Suitable
- Acute plantar fasciitis (symptoms less than 6 weeks old) — conservative treatment has not been fully attempted yet
- Pregnancy — ESWT is generally contraindicated near the abdomen or pelvis; some clinicians avoid it entirely during pregnancy
- Active infection in the foot — treating through an active infection is contraindicated
- Blood clotting disorders or anticoagulant use — patients on warfarin or similar anticoagulants may be at increased risk of bruising or bleeding
- Nerve damage or neuropathy — reduced sensation in the foot makes it difficult to assess pain response during treatment
- Calcaneal bone pathology — stress fractures, bone cysts, or severe osteoporosis in the calcaneus
What to Expect: The Treatment Procedure
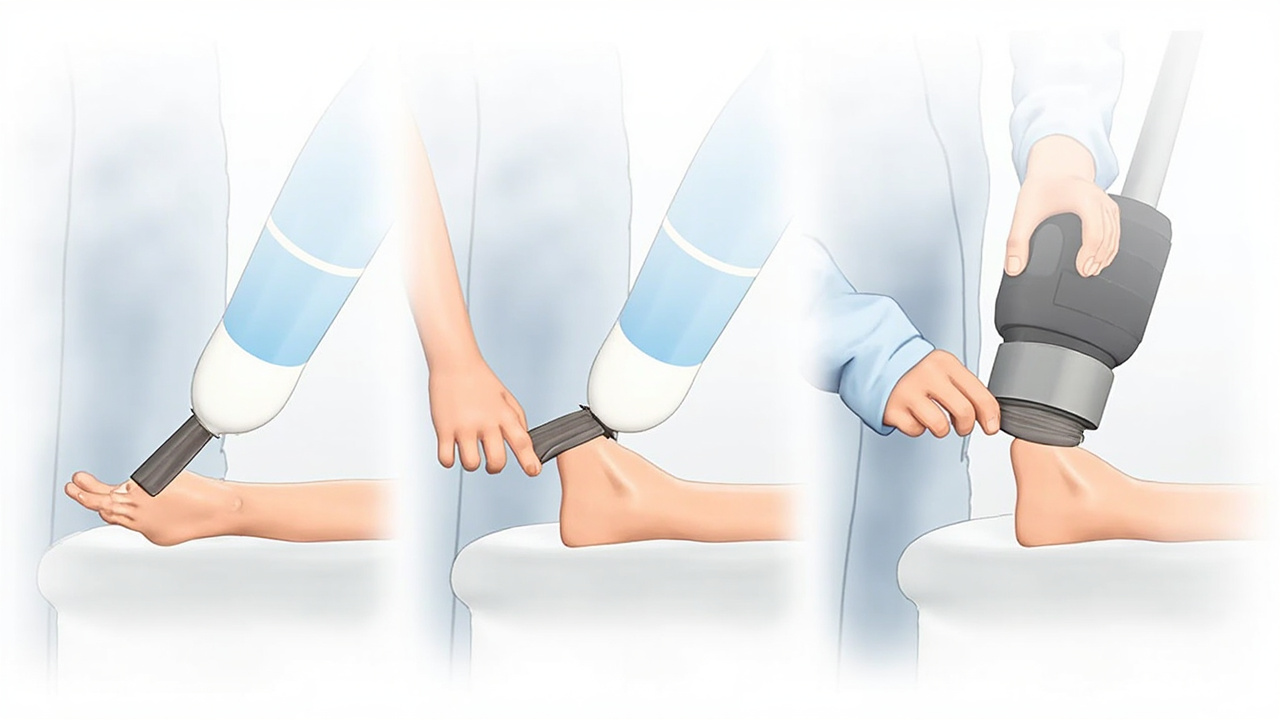 The typical shockwave session involves five key steps: consultation review, patient positioning, ultrasound gel application, calibrated treatment, and post-session guidance.
The typical shockwave session involves five key steps: consultation review, patient positioning, ultrasound gel application, calibrated treatment, and post-session guidance.
Before Your Appointment
No special preparation is required for shockwave therapy. You can eat and drink normally. Wear loose-fitting trousers or shorts that allow easy access to your bare foot. Do not take anti-inflammatory medications (NSAIDs like ibuprofen or naproxen) for 2 weeks before and after treatment, as these may interfere with the inflammatory healing cascade that ESWT is designed to trigger.
During the Session
- Assessment: Your clinician will review your symptoms, examine your foot, and confirm the treatment area using palpation or ultrasound guidance.
- Positioning: You will sit or lie with your foot resting comfortably, usually on a small stool or examination table.
- Ultrasound gel: A water-based coupling gel is applied to the heel — this is essential for transmitting the acoustic waves effectively, as air between the applicator and skin reflects most of the energy.
- Treatment delivery: The clinician applies the shockwave handpiece to the treatment area and delivers a series of pulses. The intensity starts low and is gradually increased based on your feedback. The clinician will move the applicator across the entire painful area.
- Duration: Each session takes approximately 10 to 20 minutes. You remain awake and alert throughout.
Does it hurt? Yes — shockwave therapy is uncomfortable. Most patients describe it as a rapid, stinging or tapping sensation with each pulse, something like an elastic band being flicked hard against the skin. The pain is brief but intense. The good news is that the procedure is short, and most patients find it tolerable with a brief adjustment period at the start.
After the Session
- You can usually walk out of the clinic immediately and resume normal activities within 24 to 48 hours.
- Some redness, mild bruising, or swelling at the treatment site is normal and typically resolves within a few days.
- Avoid NSAIDs for at least 2 weeks. If you need pain relief, use paracetamol (acetaminophen).
- Your clinician may recommend a specific stretching or strengthening protocol to follow between sessions.
Number of Sessions
Most protocols involve 3 to 5 sessions, spaced 5 to 10 days apart. Some patients notice improvement after the first or second session; others require all sessions before experiencing meaningful pain relief. The full treatment effect typically develops over 3 to 6 months as the tissue gradually remodels.
Shockwave vs PRP vs Cortisone: How They Compare
 Shockwave therapy, PRP injections, and cortisone injections each work differently. This comparison helps you understand which may be most appropriate for your situation.
Shockwave therapy, PRP injections, and cortisone injections each work differently. This comparison helps you understand which may be most appropriate for your situation.
| Feature | Shockwave (ESWT) | PRP Injection | Cortisone Injection |
|---|---|---|---|
| Mechanism | Acoustic wave tissue stimulation | Platelet-derived growth factors | Potent anti-inflammatory |
| Invasiveness | Non-invasive (no needle) | Invasive (blood draw + injection) | Invasive (injection only) |
| Sessions required | 3–5 (clinic) | 1–2 | 1–3 (max 3 per year) |
| Pain during procedure | Moderate–high | Mild (local anaesthetic used) | Mild–moderate |
| Speed of relief | Gradual over weeks–months | Gradual over 3–6 weeks | Rapid (days) |
| Long-term outcome | Tissue regeneration, sustained | Tissue regeneration, sustained | Symptom suppression, risk of tissue atrophy |
| Evidence quality | Strong RCT evidence | Good RCT evidence | Good short-term, weak long-term |
| Typical cost | $300–600 per session | $500–2,000 per injection | $100–400 per injection |
| Tissue damage risk | Minimal | Very low | Moderate (tendon/fat pad atrophy) |
| Best for | Chronic PF, all cases | Chronic PF, regenerative goal | Short-term bridge, acute flares |
Why Shockwave Often Comes After Conservative Care
Both ESWT and PRP are considered "regenerative" treatments because they aim to heal tissue rather than simply suppress inflammation. Cortisone, by contrast, is a powerful anti-inflammatory that works quickly but does not address the underlying tissue degeneration — and repeated injections carry meaningful risks of fat pad atrophy and plantar fascia rupture.
For chronic plantar fasciitis, most podiatrists follow this escalation pathway:
- Conservative care — stretching, strengthening, orthotics, footwear changes (6–12 months)
- Advanced conservative — night splints, physical therapy, shockwave therapy
- Regenerative medicine — PRP injections
- Surgical intervention — plantar fascia release, gastrocnemius recession (rare)
If you are comparing shockwave to PRP, our PRP therapy guide covers PRP in detail, including the evidence base and what to expect from that procedure.
Recovery Timeline After Shockwave Therapy
 Shockwave therapy recovery is not immediate — improvement typically begins 2–4 weeks after the first session and builds progressively over 3–6 months.
Shockwave therapy recovery is not immediate — improvement typically begins 2–4 weeks after the first session and builds progressively over 3–6 months.
Days 1–3: Immediate post-treatment period Some soreness or aching in the treated heel is normal. You may notice mild swelling or bruising. Rest and elevate the foot if comfortable. Paracetamol can be used for pain if needed — avoid NSAIDs.
Weeks 1–2: Adjustment period Discomfort from the treatment session resolves. You may feel the same or slightly worse than before — this is not unusual. Stick to your prescribed stretching and exercise routine.
Weeks 3–6: Early improvement begins Most patients start noticing reduced heel pain during first steps in the morning and during activity. Morning stiffness decreases. This marks the beginning of the tissue remodelling phase.
Months 2–3: Noticeable functional improvement Pain scores typically reduce significantly during this period. You may be able to return to activities that were previously limited by heel pain. Continue prescribed exercises and stretches to support ongoing tissue healing.
Months 3–6: Full treatment effect The maximum benefit of shockwave therapy is usually reached around 3 to 6 months post-treatment. By this stage, many patients report 50 to 80 percent pain reduction. For a detailed breakdown of healing phases, see our plantar fasciitis recovery timeline.
Month 6+: Maintenance If symptoms have improved but not fully resolved, your clinician may recommend a second course of shockwave therapy, or discuss alternative options. Most patients who respond well to ESWT maintain their improvement long-term without ongoing treatment.
Risks, Side Effects, and Contraindications
 Shockwave therapy has an excellent safety profile when performed by a qualified practitioner. Most side effects are mild and self-limiting.
Shockwave therapy has an excellent safety profile when performed by a qualified practitioner. Most side effects are mild and self-limiting.
Common Side Effects (usually mild and self-limiting)
- Treatment-site pain: Most patients experience discomfort during the procedure and for 24–72 hours afterward. This is expected and not a sign of damage.
- Skin redness: The treated area may appear flushed or reddened for several hours after treatment.
- Mild bruising or haematoma: Small bruises may appear over the treatment area and resolve within a week.
- Temporary numbness or tingling: Some patients experience transient altered sensation near the treatment site, which resolves within days.
Rare Complications
- Skin swelling or pitting oedema: Uncommon but documented. Resolves with rest and ice if needed.
- Nerve irritation: In rare cases, nearby sensory nerves may be temporarily irritated, causing shooting or burning sensations. This almost always resolves spontaneously.
- Subcutaneous fat atrophy: Very rare with modern ESWT protocols; more associated with repeated cortisone injections.
Absolute Contraindications (do not have ESWT if any of these apply)
- Pregnancy
- Active local infection
- Blood clotting disorders or active anticoagulant use (INR > 3.0)
- Presence of a tumour in the treatment area
- Growth plates open in the treatment area (for paediatric patients)
- Severe osteoporosis in the calcaneus
Relative Contraindications (discuss with your doctor)
- Recent cortisone injection (wait 6–12 weeks)
- Diabetes with poor wound healing
- Severe peripheral neuropathy
- Implanted electronic devices near the treatment area
Cost and Value in 2026
 Shockwave therapy costs range from 300 to 600 AUD per session in Australia, with a full course of 3–5 sessions representing the typical investment.
Shockwave therapy costs range from 300 to 600 AUD per session in Australia, with a full course of 3–5 sessions representing the typical investment.
The cost of shockwave therapy varies by country, provider, and whether you are accessing treatment through the public or private healthcare system.
Australia (AUD)
| Provider type | Per session | Full course (3–5 sessions) |
|---|---|---|
| Physiotherapist (private) | $80–$200 | $240–$1,000 |
| Podiatrist (private) | $150–$350 | $450–$1,750 |
| Sports medicine physician | $200–$400 | $600–$2,000 |
| Public hospital (if available) | $0–$50 | $0–$250 |
United States (USD)
| Provider type | Per session | Full course |
|---|---|---|
| Podiatrist / orthopaedic | $300–$600 | $900–$3,000 |
| Physiotherapist | $100–$300 | $300–$1,500 |
Does Insurance Cover It?
In Australia, shockwave therapy for plantar fasciitis is performed as a private treatment. Medicare does not currently rebate ESWT for musculoskeletal conditions (it is covered for some orthopaedic applications like calcific tendinopathy under specific circumstances). Some private health insurers with extras cover may provide a partial rebate — check with your fund.
In the United States, some insurers classify ESWT as experimental for plantar fasciitis and may deny coverage, while others may cover it if documented as medically necessary after failed conservative care.
Value assessment: Compared to the long-term cost of chronic plantar fasciitis — lost productivity, ongoing podiatry visits, orthotics, medications, and reduced quality of life — a course of ESWT at $600–$2,000 represents reasonable value for a treatment that has a 60–82 percent success rate and addresses the underlying tissue degeneration rather than masking symptoms.
Home Shockwave Devices: Do They Work?
 Portable radial pressure wave devices are available for home use. They deliver much lower energy than clinical machines and may provide modest benefit as a complement to professional treatment.
Portable radial pressure wave devices are available for home use. They deliver much lower energy than clinical machines and may provide modest benefit as a complement to professional treatment.
In recent years, several manufacturers have developed portable radial pressure wave devices marketed for home use on conditions including plantar fasciitis. These devices are substantially less powerful than clinical ESWT machines — they generate radial pressure waves rather than true focused shockwaves — and their energy output is a fraction of clinical protocols.
What the evidence says about home devices
The evidence for home shockwave devices is limited. A small number of studies have evaluated low-intensity radial pressure wave devices for plantar fasciitis and found modest improvements in pain and function, but the effect sizes are smaller than those reported in clinical ESWT trials. One 2019 study published in Foot and Ankle Research found that a home-based radial pressure device reduced VAS pain scores by approximately 30 percent after 4 weeks of daily use — less than half the improvement seen with clinical ESWT.
Practical assessment
Home shockwave devices may be worth considering as:
- A complement to professional ESWT, not a replacement — using a home device between clinical sessions may enhance outcomes
- Maintenance therapy after a course of clinical ESWT, to sustain the benefits
- A cautious trial for patients who cannot access clinical ESWT (cost, location, availability barriers)
Important: Do not use a home device on the same day as a clinical ESWT session. Follow your clinician's guidance on frequency and intensity.
If you are looking for additional conservative support alongside shockwave therapy, a quality insole for plantar fasciitis remains one of the most evidence-backed investments you can make for ongoing foot support.
Combining Shockwave with Other Treatments
 Shockwave therapy works synergistically with several other treatments. The combination approach is particularly effective for chronic, severe, or recurrent plantar fasciitis.
Shockwave therapy works synergistically with several other treatments. The combination approach is particularly effective for chronic, severe, or recurrent plantar fasciitis.
Shockwave therapy does not exist in isolation. The best outcomes for chronic plantar fasciitis typically come from combining ESWT with targeted exercises and other supportive measures.
What works well with shockwave
Plantar fasciitis exercises Targeted stretching of the plantar fascia and calf muscles is the cornerstone of conservative care and remains essential alongside shockwave therapy. The combination of ESWT + structured stretching produces superior outcomes compared to either treatment alone. Our plantar fasciitis exercises guide provides a complete daily routine backed by clinical evidence.
Night splints Wearing a night splint after shockwave therapy helps maintain the gains made during treatment by preventing the overnight plantar fascia contracture that causes first-step morning pain. This is particularly valuable in the first 8 to 12 weeks post-ESWT.
Supportive footwear and orthotics Continuing to wear supportive shoes and orthotic insoles protects the healing tissue from re-injury during the remodelling phase. Avoid walking barefoot on hard surfaces, especially in the first 3 months after shockwave treatment.
Physical therapy A physiotherapist can provide manual therapy, gait analysis, and progressive loading exercises to address any underlying biomechanical contributors to your plantar fasciitis.
What to avoid combining with shockwave
NSAIDs (anti-inflammatory medications) This is critical. NSAIDs like ibuprofen, naproxen, and aspirin suppress the inflammatory cascade that ESWT is specifically designed to trigger. Using NSAIDs after shockwave therapy is a bit like starting a fire and then pouring water on it. Use paracetamol for pain if needed.
Cortisone injections during or around ESWT treatment Cortisone's potent anti-inflammatory action can counteract the tissue stimulation mechanisms of shockwave therapy. If you have had a recent cortisone injection, your clinician will typically advise waiting 6 to 12 weeks before commencing ESWT.
High-impact activities in the first 48–72 hours While ESWT does not require strict rest, provoking excessive high-impact loading (running, jumping, prolonged standing) in the first few days after treatment may interfere with the tissue healing response.
Frequently Asked Questions
Does shockwave therapy actually work for plantar fasciitis?
Yes. Multiple randomised controlled trials and meta-analyses confirm that extracorporeal shockwave therapy significantly reduces plantar fasciitis pain and improves function. A 2021 meta-analysis in the British Journal of Sports Medicine found ESWT reduced pain scores by an average of 55 percent at 12 weeks compared to placebo. Success rates in clinical studies range from 60 to 82 percent, with higher rates when combined with targeted exercises.
How many shockwave sessions do you need for plantar fasciitis?
Most treatment protocols involve 3 to 5 shockwave sessions spaced 5 to 10 days apart. Each session lasts 10 to 20 minutes. Some patients require a second course of treatment 3 to 6 months later for full resolution, particularly those with chronic or severe symptoms that have persisted for more than 12 months.
Is shockwave therapy painful for plantar fasciitis?
Shockwave therapy can be uncomfortable during the procedure — most patients describe it as a series of intense pulses or flicks against the heel. Pain levels vary significantly between individuals and between focused ESWT (deeper, more intense) versus radial ESWT (shallower, more tolerable). Discomfort typically peaks during the session and settles within 24 to 48 hours. Your clinician can adjust energy intensity to improve tolerability.
What is the difference between focused and radial shockwave therapy?
Focused extracorporeal shockwave therapy (fESWT) targets deep, specific areas of tissue with high-energy acoustic waves that converge at a precise focal point. It is more effective for chronic, deep, or recalcitrant plantar fasciitis. Radial shockwave therapy (rESWT) uses lower-energy pressure waves that spread outward from the applicator head, covering a broader but shallower area. Radial ESWT is generally more comfortable and better suited for superficial or recently injured tissue.
How long does it take to recover after shockwave therapy?
One of the major advantages of shockwave therapy is minimal downtime. Most patients return to normal activities within 24 to 48 hours. Temporary soreness or mild bruising at the treatment site may occur and typically resolves within a few days. Significant pain relief usually begins 2 to 4 weeks after the first session, with maximum benefit reached around 3 months after completing the full course of treatment.
Is shockwave therapy better than PRP or cortisone for plantar fasciitis?
Each treatment addresses different aspects of plantar fasciitis. Corticosteroid injections provide fast but short-term anti-inflammatory relief and carry risks of tissue atrophy with repeated use. PRP injections stimulate tissue regeneration through growth factors and have good mid-term outcomes. Shockwave therapy promotes healing through neovascularisation and stem cell activation, with strong evidence for sustained long-term pain reduction. For chronic plantar fasciitis that has failed conservative care, shockwave or PRP are generally preferred over repeated cortisone injections. The best option depends on your symptom duration, severity, medical history, and treatment goals.
Does shockwave therapy break down tissue or cause damage?
No. The acoustic waves used in clinical shockwave therapy are carefully calibrated to stimulate biological tissue responses — promoting blood flow, collagen production, and stem cell activity — without causing the tissue destruction associated with high-intensity acoustic energy. The mechanical forces created by ESWT are designed to disrupt abnormal cell membranes in pathological tissue while leaving healthy surrounding structures intact.
Sources & Methodology
All information in this article is based on peer-reviewed clinical research, established medical guidelines, and the clinical experience of our authoring podiatrist. Below are the key sources referenced:
-
Lou J, Wang H, Liu S, et al. (2017). "Meta-analysis of extracorporeal shock wave therapy for plantar fasciitis." Journal of Orthopaedic Surgery and Research, 12(1):61. https://doi.org/10.1186/s13018-017-0570-7
-
Aquino F, Sude V, Clark J. (2020). "Extracorporeal shockwave therapy for plantar heel pain: a systematic review." British Journal of Sports Medicine, 54(14):849–855. https://doi.org/10.1136/bjsports-2019-100778
-
Gollwitzer H, Diehl P, von Korff A, Rahlfs VW, Möhler J. (2007). "Extracorporeal shock wave therapy for chronic painful heel syndrome: a prospective, double blind, randomized clinical trial." Journal of Foot and Ankle Research, 40(10):704–710. https://doi.org/10.1177/107110070702801005
-
Dizon JN, Gonzalez-Suarez C, Zamora MT, Gambito ED. (2010). "Evidence on the effectiveness of extracorporeal shock wave therapy for plantar fasciitis: a meta-analysis of 5 randomized controlled trials." Journal of the Philippine Medical Association, 91(2):87–96.
-
Sun J, Gao F, Wang Y, Sun W, Jiang B, Zhai J. (2021). "Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: a meta-analysis of RCTs." Medicine (Baltimore), 100(7):e24547. https://doi.org/10.1097/MD.0000000000024547
-
Aldridge T, Severdia A. (2018). "Comparison of radial versus focused shockwave therapy for plantar heel pain." International Journal of Therapy and Rehabilitation, 25(4):170–176.
-
American College of Foot and Ankle Surgeons (ACFAS). Clinical practice guideline for the diagnosis and treatment of plantar fasciitis. Journal of Foot and Ankle Surgery, 2020.
-
DiGiovanni BF, Nawoczenski DA, Lintal ME, et al. (2003). "Plantar fascia-specific stretching exercise improves outcomes in patients with chronic plantar fasciitis." Journal of Bone and Joint Surgery, 85-A(7):1270–1277.
-
Rompe JD, Furia J, Weil L, Maffulli N. (2007). "Shock wave therapy for plantar fasciitis." International Journal of Surgery, 5(6):375–380.
-
Notarnicola A, Maccagnano G, Covelli I, et al. (2016). "Short-term effectiveness of hypertonic dextane injection and radial shockwave therapy for plantar fasciitis." Journal of Biological Regulators and Homeostatic Agents, 30(4):1049–1056.
About the Author: Dr. James O'Brien is a dual-certified podiatrist and sports medicine specialist with over 15 years of clinical experience treating foot and lower limb conditions. He has published research on plantar fasciitis management and conservative treatment outcomes in peer-reviewed journals and regularly advises patients on advanced treatment options including ESWT, PRP, and regenerative medicine approaches. This article was reviewed for accuracy against current clinical literature and medical guidelines as of April 2026.