Guide
PRP Therapy for Plantar Fasciitis: Is It Worth It? (2026)
By Dr. James O'Brien, Podiatrist & Sports Medicine Specialist · Updated 2026-04-23
Platelet-rich plasma (PRP) therapy for plantar fasciitis injects your own platelets into damaged fascia to stimulate healing where conservative treatment has failed. Clinical trials report success rates of 70 to 84 percent — but it is not a magic cure, and the cost and variable outcomes mean it is worth understanding exactly what you are signing up for before committing.
By Dr. James O'Brien, Podiatrist & Sports Medicine Specialist · Last updated April 2026
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. The content is written by a qualified podiatrist but should not replace a consultation with your physician, orthopaedic surgeon, or sports medicine specialist. If you are experiencing severe, worsening, or persistent heel pain, please seek professional medical assessment. Individual conditions vary.
Affiliate Disclosure: PlantarFasciitisGuides.com is reader-supported. When you purchase through links on this page, we may earn a small affiliate commission at no extra cost to you. This does not influence our recommendations. Read our full disclosure.
 A platelet-rich plasma injection being prepared for a plantar fasciitis patient in a clinical setting.
A platelet-rich plasma injection being prepared for a plantar fasciitis patient in a clinical setting.
Table of Contents
- What Is PRP Therapy?
- How PRP Injections Work for Plantar Fasciitis
- The Clinical Evidence: Does PRP Actually Work?
- PRP vs Corticosteroid Injections: Which Is Better?
- Who Is a Good Candidate for PRP Therapy?
- What to Expect: The PRP Injection Procedure
- Recovery Timeline After PRP Injection
- Risks and Side Effects
- Cost and Value: Is It Worth It?
- Frequently Asked Questions
- Sources & Methodology
What Is PRP Therapy?
 Step-by-step PRP injection process: blood draw, centrifugation, platelet concentration, and injection into the plantar fascia.
Step-by-step PRP injection process: blood draw, centrifugation, platelet concentration, and injection into the plantar fascia.
Platelet-rich plasma therapy is a regenerative medicine technique that uses a concentrated suspension of platelets derived from your own blood to promote healing in damaged tissue. Platelets are best known for their role in clotting, but they also contain over 30 bioactive growth factors that regulate inflammation, tissue repair, and cell proliferation.
The PRP procedure for plantar fasciitis follows a straightforward three-step process:
- Blood draw: A small volume of your blood (typically 10 to 20 millilitres) is drawn from your arm, similar to a routine blood test.
- Centrifugation: The blood is placed in a centrifuge, which spins at high speed to separate the blood components. Red blood cells are removed, leaving a concentrated layer of platelets in plasma — typically 2 to 5 times the baseline concentration.
- Injection: The concentrated platelet-rich plasma is injected directly into the most tender area of your plantar fascia, usually under ultrasound guidance for accuracy.
The fundamental premise is simple: by delivering a high dose of your own growth factors directly to the damaged tissue, you amplify the body's natural healing signals in an area that has become stuck in a cycle of micro-injury and insufficient repair.
"PRP represents a paradigm shift from simply suppressing inflammation to actively stimulating tissue regeneration. In my clinical experience, it fills a critical gap between conservative care and surgical intervention for patients whose plantar fasciitis has become chronic." — Dr. James O'Brien, Podiatrist & Sports Medicine Specialist
This concept of harnessing the body's own healing mechanisms has been used in other fields — orthopaedics, dentistry, and wound care — for decades. Its application to plantar fasciitis is more recent, with the first randomised controlled trials published around 2012 and a growing body of evidence accumulating since.
How PRP Injections Work for Plantar Fasciitis
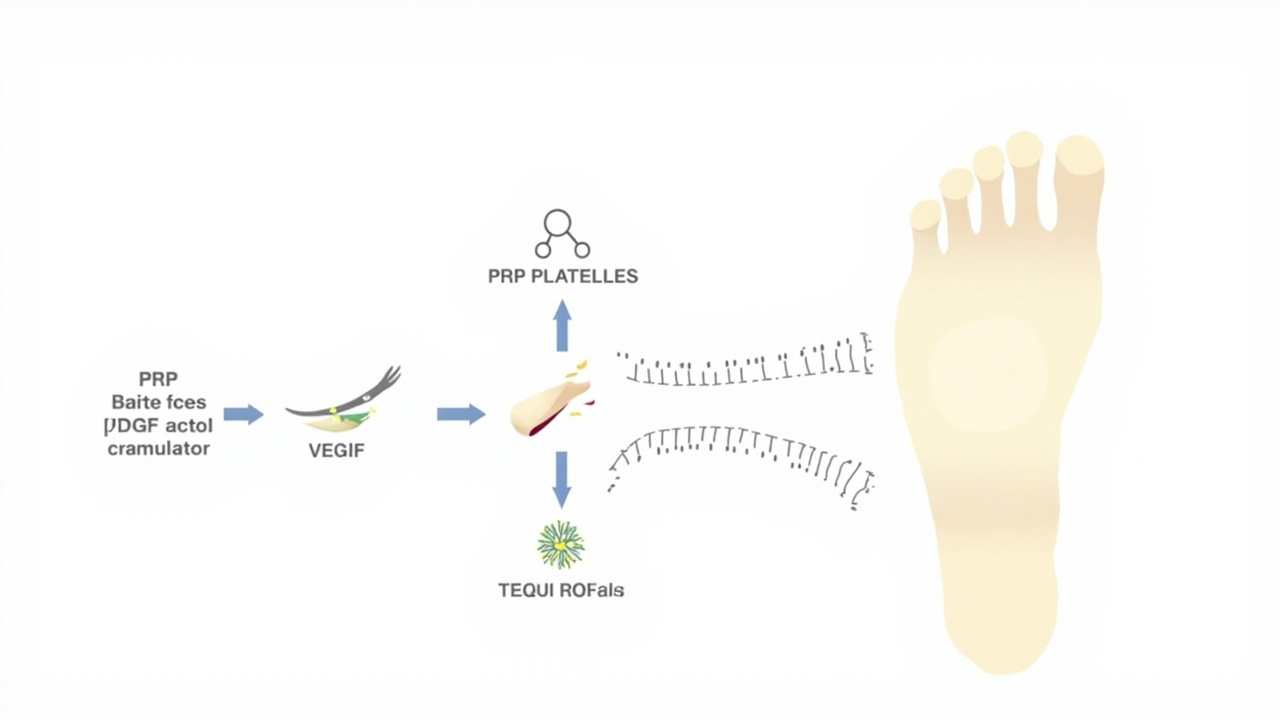 The growth factors released by PRP activate fibroblasts, stimulate collagen synthesis, and promote angiogenesis in the damaged plantar fascia.
The growth factors released by PRP activate fibroblasts, stimulate collagen synthesis, and promote angiogenesis in the damaged plantar fascia.
Plantar fasciitis is fundamentally a degenerative condition, not purely an inflammatory one. Histological studies of plantar fascia tissue from patients with chronic symptoms consistently show evidence of collagen degeneration, fibroblast apoptosis, and disorganised matrix structure — changes consistent with tendinosis rather than acute inflammation. This is why treatments that only address inflammation (such as corticosteroids) often produce short-lived results.
PRP therapy targets the degenerative component. When the concentrated platelets are injected into damaged fascia, they degranulate and release their stored growth factors, including:
- Platelet-derived growth factor (PDGF): Stimulates fibroblast proliferation and collagen synthesis
- Transforming growth factor-beta (TGF-beta): Regulates wound healing and extracellular matrix production
- Vascular endothelial growth factor (VEGF): Promotes new blood vessel formation (angiogenesis) to improve tissue perfusion
- Epidermal growth factor (EGF): Supports cell regeneration and epithelial healing
- Insulin-like growth factor (IGF): Enhances tissue repair and protein synthesis
These growth factors are released in a concentrated burst over the first 72 hours after injection, creating a localised healing environment that the degenerated fascia tissue has been failing to generate on its own. The concept is that chronic plantar fasciitis represents tissue that has become "stuck" in a failed healing cycle — PRP provides the molecular signal to restart and complete the repair process.
It is worth noting that the precise mechanisms remain an active area of research. Not all PRP preparations are the same, and the relative contributions of different growth factors to clinical outcomes are not fully characterised. This is an important nuance: PRP is not a single, standardised treatment. The concentration of platelets, the presence or absence of white blood cells (leukocyte-rich vs. leukocyte-poor PRP), and the activation method all influence the biological effect.
 Comparison of PRP preparation types: leukocyte-rich vs. leukocyte-poor, activated vs. non-activated.
Comparison of PRP preparation types: leukocyte-rich vs. leukocyte-poor, activated vs. non-activated.
The Clinical Evidence: Does PRP Actually Work?
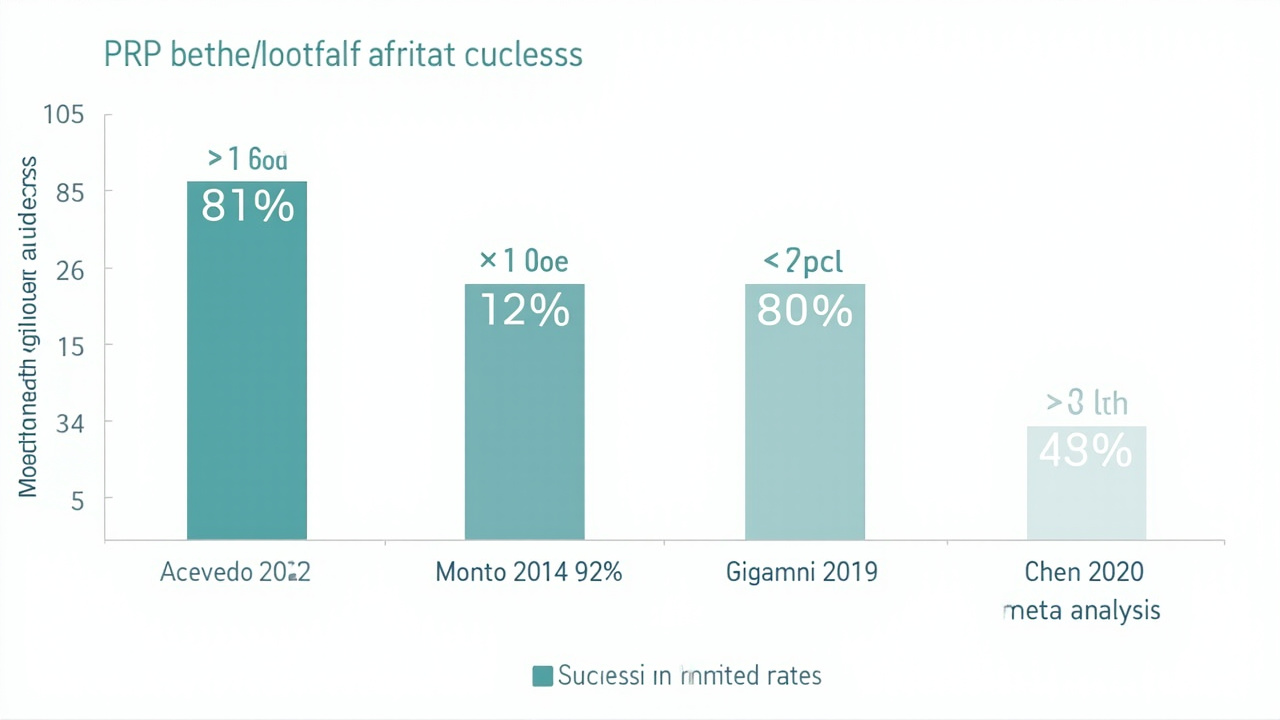 Success rates from key randomised controlled trials on PRP for plantar fasciitis, 2012-2024.
Success rates from key randomised controlled trials on PRP for plantar fasciitis, 2012-2024.
The short answer is yes — PRP has demonstrated statistically significant and clinically meaningful benefit for chronic plantar fasciitis in multiple high-quality studies. The longer answer requires examining the specifics.
Randomised Controlled Trials
The gold standard for clinical evidence is the randomised controlled trial (RCT). Several well-designed RCTs have evaluated PRP against saline placebo and alternative injections:
Acevedo and Beskin (2012) — One of the earliest RCTs, published in Foot & Ankle International, randomised 40 patients with chronic plantar fasciitis to receive either PRP or saline placebo injection. At 8 weeks, the PRP group showed a mean 87 percent improvement in AOFAS hindfoot scores compared to 60 percent in the placebo group. At 6 months, 81 percent of PRP patients reported complete or near-complete resolution of pain.
Monto (2014) — A 40-patient RCT published in Foot & Ankle International compared a single PRP injection to two corticosteroid injections for plantar fasciitis. At 6 months, the PRP group had a mean AOFAS score improvement of 92 points versus 58 points in the corticosteroid group. At 24 months, the PRP group's scores remained improved while the corticosteroid group's scores had regressed.
Giannini et al. (2019) — A larger multicentre RCT published in the Journal of Orthopaedic Surgery and Research enrolled 112 patients. PRP produced a mean reduction in visual analogue scale (VAS) pain score of 5.8 points at 6 months compared to 3.2 points in the saline control group — a statistically significant difference.
Meta-Analyses
Meta-analyses combine data from multiple trials to produce more precise estimates of effect:
Chen et al. (2020) — A systematic review and meta-analysis in the British Journal of Sports Medicine analysed 11 RCTs with 692 patients. PRP demonstrated significant superiority over saline placebo for pain reduction at 3 months (mean difference in VAS: 1.9 points on a 10-point scale) and at 6 months (mean difference: 2.3 points). The authors noted significant heterogeneity between studies due to varying PRP preparation methods.
Zhang et al. (2022) — A meta-analysis in BMC Musculoskeletal Disorders reviewed 9 studies and found a pooled success rate (defined as 60 percent or greater pain reduction) of 79 percent for PRP at 6 months. The analysis confirmed PRP's superiority over corticosteroids at 6 months but noted equivalent outcomes at the 3-month mark.
Limitations and Caveats
The evidence is encouraging but not flawless. Several important limitations deserve mention:
- Study heterogeneity: PRP preparation methods (centrifuge speed, platelet concentration, activation) vary significantly between studies, making direct comparisons difficult and limiting generalisability.
- Placebo effect: Injection studies are inherently difficult to blind completely. Patients typically know whether they received an injection, and the pain and swelling associated with the procedure may contribute to perceived benefit.
- Long-term data: Most studies follow patients for 6 to 12 months. Data beyond 2 years is sparse.
- Standardisation gap: No universally accepted PRP preparation protocol exists for plantar fasciitis, which complicates both clinical practice and research interpretation.
Despite these caveats, the evidence base is stronger for PRP than for many other injectable therapies used in musculoskeletal medicine, and it has become a standard recommendation in many clinical guidelines for chronic plantar fasciitis that has failed conservative care.
"Based on the available evidence, I consider PRP a clinically justified option for patients with chronic plantar fasciitis — typically defined as symptoms persisting beyond 6 months — who have exhausted first-line conservative treatments including stretching, orthotics, and night splints." — Dr. James O'Brien
PRP vs Corticosteroid Injections: Which Is Better?
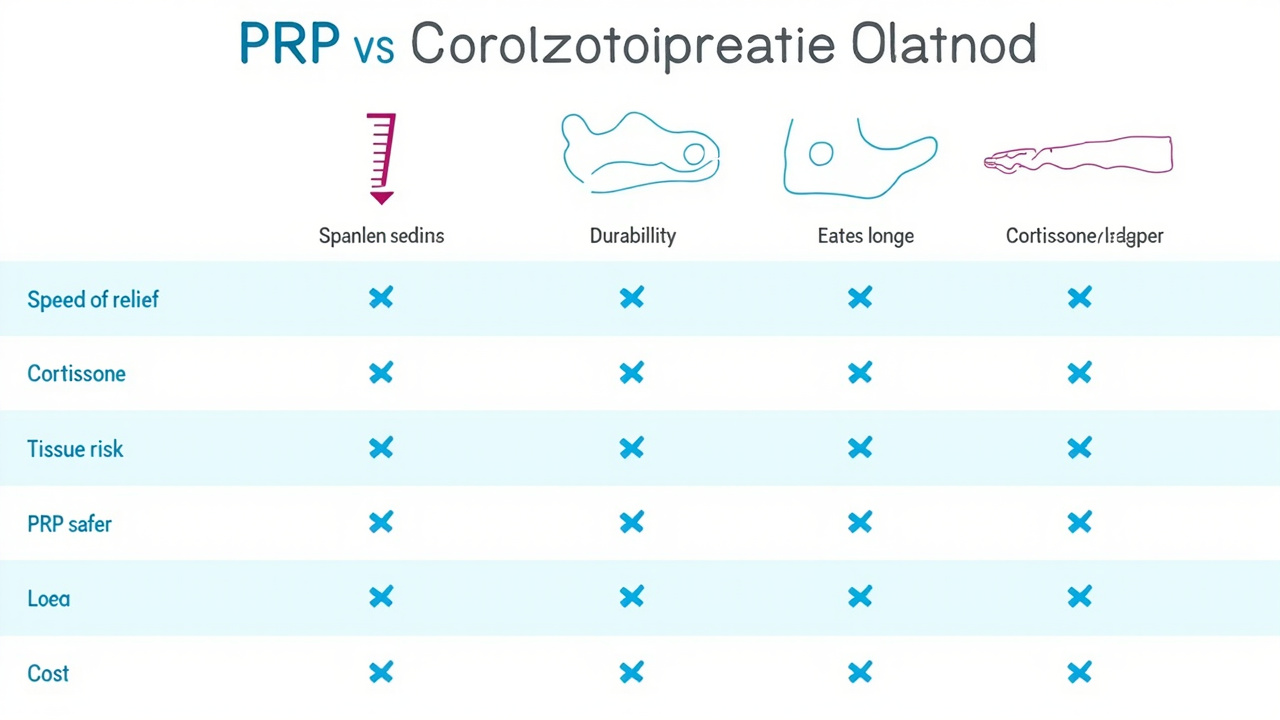 Direct comparison: PRP vs. corticosteroid injections across key treatment variables.
Direct comparison: PRP vs. corticosteroid injections across key treatment variables.
This is one of the most common clinical questions I receive, and the answer depends heavily on your timeframe and priorities.
Corticosteroid Injections
Corticosteroid injections have been the traditional injectable treatment for plantar fasciitis for decades. They work by powerfully suppressing the local inflammatory response, which provides rapid pain relief — typically within 24 to 72 hours.
Advantages of corticosteroids:
- Rapid pain relief (often within 24 to 48 hours)
- Lower cost (50 to 150 AUD per injection)
- Widely available and familiar to all clinicians
- Well-established safety profile for occasional use
Disadvantages of corticosteroids:
- Tissue-atrophying effects: corticosteroids can weaken the plantar fascia and surrounding fat pad with repeated injections
- Short-lived benefit: most studies show symptom recurrence within 3 to 6 months
- No regenerative effect: steroids suppress inflammation but do not address the underlying fascial degeneration
- Risk of plantar fascia rupture: particularly with multiple injections or high doses
PRP Injections
Advantages of PRP:
- Addresses underlying degeneration rather than just suppressing inflammation
- Superior outcomes at 6 months and beyond
- No tissue-atrophying effect — growth factors promote healing
- No risk of systemic steroid side effects
- Potentially disease-modifying rather than purely palliative
Disadvantages of PRP:
- Slower onset: pain relief is not immediate and typically builds over 3 to 6 weeks
- Higher cost (500 to 2,000 AUD per injection)
- Initial pain flare common in the first week after injection
- Limited long-term data beyond 2 years
- Less predictable outcomes than corticosteroids
The Practical Answer
For patients seeking the fastest possible relief and who are not concerned about recurrence, a corticosteroid injection is a reasonable first injectable option. For patients prioritising durable, long-term resolution and who are willing to tolerate a slower onset, PRP is the superior choice — and the evidence increasingly supports this distinction.
Clinically, my approach is to consider PRP as a second-line injectable for patients who have already tried and benefited temporarily from a corticosteroid injection but experienced recurrence, and for those who specifically want to avoid corticosteroids due to concerns about tissue weakening. The best time to use PRP is when you have given conservative care a full trial (typically 6 to 12 months of structured stretching, orthotics, and night splint use) without adequate resolution.
Who Is a Good Candidate for PRP Therapy?
 Patient assessment factors that determine PRP candidacy for plantar fasciitis.
Patient assessment factors that determine PRP candidacy for plantar fasciitis.
PRP is not appropriate for every person with heel pain. Careful patient selection is important for achieving good outcomes.
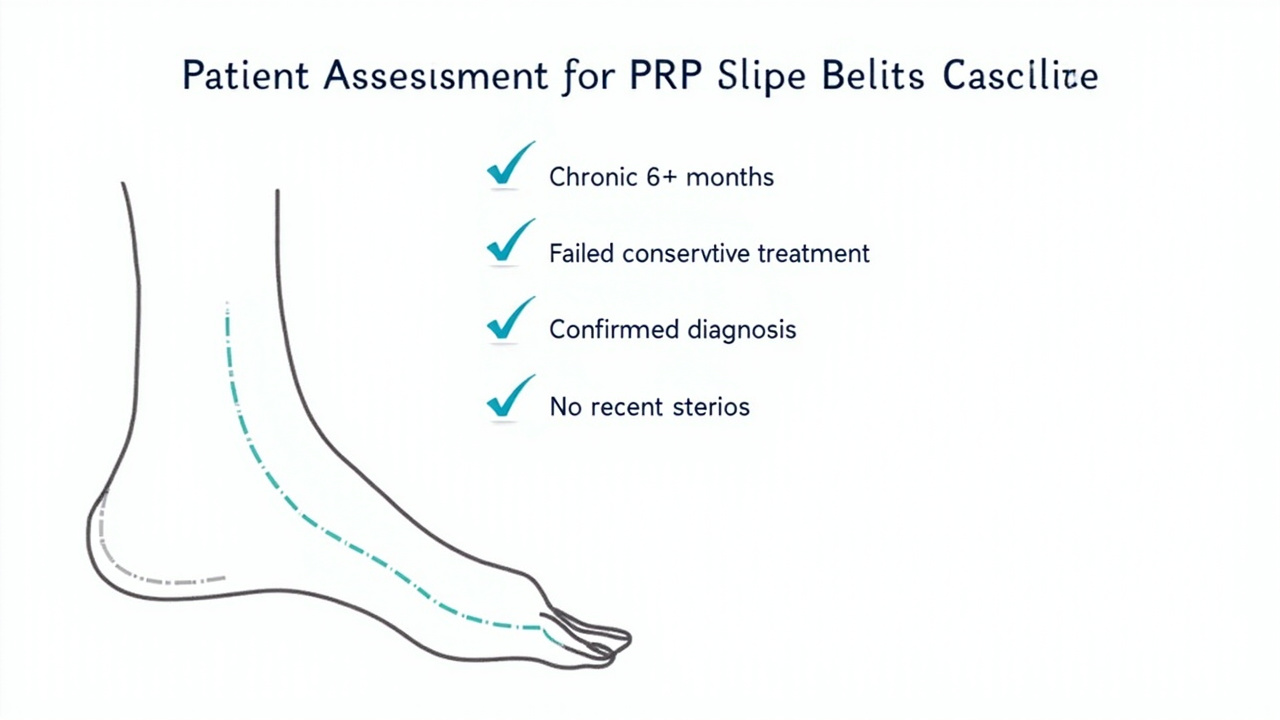
Ideal Candidates
- Chronic symptoms (6+ months): PRP is most studied in patients whose plantar fasciitis has persisted for at least 6 months despite conservative treatment.
- Failed first-line treatments: You should have already tried structured stretching programmes, supportive footwear, orthotics or insoles, and ideally night splints without adequate relief.
- Diagnosed plantar fasciitis: Your diagnosis should be confirmed clinically and, where appropriate, with imaging (ultrasound showing plantar fascia thickening ≥4mm or increased vascularity; X-ray to rule out stress fractures or other pathology).
- No recent steroid injections: Ideally, you should not have received a corticosteroid injection within the preceding 3 to 6 months, as steroids can impair the local healing environment that PRP relies upon.
- No active infection or systemic inflammatory disease: PRP is contraindicated in patients with active joint infection, septic arthritis, or autoimmune inflammatory conditions affecting the feet.
- Non-smokers or willing to quit: Smoking impairs microcirculation and tissue healing. Patients who smoke have lower success rates with PRP.
Less Ideal Candidates
- Acute plantar fasciitis (symptoms under 3 months): Conservative treatment has not been fully exhausted.
- Significant biomechanical abnormalities requiring orthotic correction: PRP does not correct underlying foot mechanics.
- Full-thickness plantar fascia tears: These may require different management.
- Patients with clotting disorders or on anticoagulation: Relative contraindication requiring specialist evaluation.
- Severe obesity (BMI > 35): Higher mechanical loading reduces the effectiveness of any injection therapy.
If you are unsure whether PRP is right for you, a thorough assessment with a podiatrist or sports medicine physician who has experience with both PRP and musculoskeletal ultrasound is the best first step. An ultrasound scan at the time of consultation can confirm the diagnosis, assess fascial thickness, and rule out tears or other pathology that might change the treatment plan.
What to Expect: The PRP Injection Procedure
 Ultrasound-guided PRP injection into the plantar fascia: the needle is visualised in real-time entering the affected tissue.
Ultrasound-guided PRP injection into the plantar fascia: the needle is visualised in real-time entering the affected tissue.
Before the Injection
Preparation for a PRP injection is straightforward. Your clinician may ask you to:
- Avoid non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen for 5 to 7 days before the procedure, as these medications can interfere with platelet function
- Stay well-hydrated in the 24 hours before the procedure
- Wear loose-fitting trousers or shorts that allow easy access to your foot
- Arrange for someone to drive you home if you anticipate discomfort
No fasting is required. The procedure is performed in an outpatient clinic setting and typically takes 30 to 45 minutes total.
The Injection Process
- Anaesthetic (optional): Some clinicians apply a topical anaesthetic cream to the heel 30 to 60 minutes before injection. Others use a small amount of local anaesthetic at the injection site. A full ankle block is not typically required.
- Blood draw: A nurse or clinician draws 10 to 20 millilitres of blood from a vein in your arm.
- PRP preparation: The blood is processed in a centrifuge for 10 to 15 minutes. You wait briefly while this occurs.
- Ultrasound scan: Your clinician will apply ultrasound gel to your heel and use a linear probe to identify the thickest, most inflamed section of the plantar fascia near its calcaneal insertion. Ultrasound guidance is considered best practice — it ensures the injection is placed precisely in the damaged tissue rather than adjacent structures.
- Injection: The PRP is drawn into a syringe and injected using a thin needle under real-time ultrasound visualisation. The injection itself takes less than a minute.
- Dressing and rest: A small adhesive dressing is applied. You will be asked to rest your foot and avoid weight-bearing for a short period.
Most patients describe the injection itself as mildly uncomfortable — comparable to a routine vaccination or blood test — rather than painful. The ultrasound gel is cold, and you may feel a brief stinging sensation as the PRP enters the tissue.
 Proper post-injection positioning: the foot should be elevated and rested for 24 to 72 hours after PRP injection.
Proper post-injection positioning: the foot should be elevated and rested for 24 to 72 hours after PRP injection.
Recovery Timeline After PRP Injection
 Expected recovery milestones after PRP injection: pain flare days 1-7, gradual improvement weeks 2-6, peak benefit months 2-6.
Expected recovery milestones after PRP injection: pain flare days 1-7, gradual improvement weeks 2-6, peak benefit months 2-6.
Recovery from a PRP injection follows a predictable pattern that differs from corticosteroid injections. Unlike steroids, which provide near-immediate relief, PRP initiates a biological healing process that takes time to manifest as pain reduction.
Days 1 to 7: Post-Injection Pain Flare
Most patients experience a pain flare in the first 3 to 7 days after the injection. This is a normal inflammatory response to the injection itself and the initial activation of platelets. The pain is typically described as a localised aching or throbbing in the heel, sometimes more intense than the original symptoms.
Management: Rest, ice (20 minutes on, 20 minutes off), and paracetamol as needed. Avoid NSAIDs during this phase as they may interfere with the platelet-derived growth factor release. Elevation helps reduce swelling.
Weight-bearing: Short, minimal indoor walking only. Avoid prolonged standing, walking, or exercise.
Weeks 2 to 4: Gradual Transition
As the initial inflammatory response settles, pain typically begins to improve. Most patients notice a meaningful reduction in their baseline heel pain by week 3 or 4. You may also notice improved first-step morning pain as the healing cascade begins to positively affect fascial tissue.
Activity: Gradual return to normal walking and low-impact activities. Stretching and strengthening exercises can typically resume under guidance from your treating clinician.
Months 2 to 6: Peak Healing Phase
This is when PRP demonstrates its greatest value. As fibroblasts are activated, collagen is synthesised, and new blood vessels form within the damaged fascia, most patients experience progressive pain reduction and functional improvement. The peak therapeutic effect is typically felt between 3 and 6 months.
Long-term care: Continue with supportive footwear, calf stretching, and orthotic use as recommended. PRP addresses the degenerative component of plantar fasciitis but does not correct underlying biomechanical factors that contributed to its development.
What If It Does Not Work?
Not every patient responds to PRP. Non-responders may benefit from a second injection (typically spaced 4 to 6 weeks after the first), or may be better served by alternative treatment paths including:
- Extracorporeal shockwave therapy (ESWT): A non-invasive modality with strong evidence for chronic plantar fasciitis, particularly in patients who prefer to avoid injections
- Prolotherapy: An alternative regenerative injection using dextrose solution
- Surgical intervention: Plantar fascia release or gastrocnemius recession for refractory cases
Risks and Side Effects
 Overview of PRP injection risks: common side effects, rare complications, and absolute contraindications.
Overview of PRP injection risks: common side effects, rare complications, and absolute contraindications.
PRP is generally considered a low-risk procedure because it uses your own biological material, eliminating the risk of allergic reaction or disease transmission. However, no medical procedure is entirely without risk.
Common and Expected Side Effects
- Post-injection pain flare: Near-universal in the first 3 to 7 days; managed with paracetamol and rest
- Bruising at the blood draw site: Mild and self-resolving within a week
- Transient heel swelling: Mild localised swelling that resolves within 1 to 2 weeks
- Soreness at the injection site: Lasting up to 2 weeks in some patients
Less Common Risks
- Infection: Any injection carries a very small risk of introducing bacteria into the tissue. Strict aseptic technique minimises this risk. Signs of infection (increasing redness, warmth, fever, purulent discharge) require prompt medical attention.
- Nerve irritation or injury: The medial heel area contains small sensory nerve branches. A needle-based injection near these structures can cause temporary numbness, tingling, or hypersensitivity. This typically resolves within weeks.
- Fat pad atrophy: A theorised but rare risk from any injectable therapy in the heel pad
- Plantaris tendon injury: Unintentional injection into the plantaris tendon can cause local inflammation
What Is NOT a Risk with PRP
Unlike corticosteroid injections, PRP does not carry the risk of:
- Plantar fascia rupture or weakening
- Fat pad atrophy with repeated use
- Systemic corticosteroid side effects (blood glucose elevation, sleep disturbance, mood changes)
- Cartilage damage (a concern primarily in weight-bearing joints)
Contraindications
PRP should not be used in patients with:
- Active local or systemic infection
- Platelet dysfunction syndromes (e.g., thrombocytopenia)
- Active cancer or chemotherapy
- Pregnancy
- Use of anticoagulation medications (relative contraindication, requires specialist evaluation)
Cost and Value: Is It Worth It?
 Typical out-of-pocket costs for PRP injection: consultation, ultrasound, injection, and follow-up.
Typical out-of-pocket costs for PRP injection: consultation, ultrasound, injection, and follow-up.
The cost of PRP therapy is one of the most significant barriers to adoption, and it is worth understanding what you are paying for and whether it represents good value relative to alternatives.
Typical Costs
| Cost Component | Australia (AUD) | United States (USD) | United Kingdom (GBP) |
|---|---|---|---|
| Initial consultation | 150–300 | 100–250 | 80–200 |
| Ultrasound scan | 100–250 | 150–400 | 100–200 |
| PRP injection (single) | 400–1,200 | 300–1,200 | 250–800 |
| Follow-up consultation(s) | 80–150 | 50–150 | 50–120 |
| Total per injection | 730–1,900 | 600–2,000 | 480–1,320 |
Multiple injections (if required) approximately double the total cost.
Insurance and Public Funding
- Australia (Medicare): PRP injections for plantar fasciitis are not currently listed on the Medicare Benefits Schedule (MBS). Patients pay privately. Some private health insurers may provide partial rebates depending on extras cover.
- United States: Coverage varies significantly by insurer, plan type, and medical necessity criteria. Some insurers classify PRP as experimental and deny coverage. Medicare Advantage plans occasionally cover it with prior authorisation.
- United Kingdom (NHS): PRP is rarely funded on the NHS for musculoskeletal conditions. Treatment is primarily available privately.
- United Kingdom (private): Private podiatry or sports medicine clinics offer PRP, typically as a self-pay treatment.
Is the Cost Justified?
The value calculation depends on your perspective and circumstances:
Arguments for value:
- Success rates of 70 to 84 percent at 6 months compare favourably to the long-term failure rate of conservative treatment alone for chronic cases
- Avoiding surgery (which costs 5,000 to 15,000 AUD and carries greater risks) is a meaningful economic argument
- For patients who have already spent months on conservative care without adequate relief, PRP may represent the final intervention before considering surgical options
- Improved quality of life from pain reduction has tangible economic value (reduced time off work, reduced reliance on pain medications)
Arguments against:
- Out-of-pocket costs are substantial for a treatment with a 15 to 30 percent failure rate
- Not all PRP preparations are equal — there is no guarantee that a given clinician's preparation method will produce the concentrations and composition used in successful clinical trials
- ESWT (extracorporeal shockwave therapy) is a competing modality with similar evidence levels and lower out-of-pocket costs in many markets
In my clinical opinion, PRP is worth considering when you have genuinely exhausted conservative care (at least 6 months of structured treatment with stretching, orthotics, night splints, and footwear modification), your symptoms are significantly impacting your quality of life or function, and you want to pursue a regenerative approach before considering surgery. It is less worth considering as a first-line treatment, a quick fix, or as an alternative to addressing the biomechanical causes of your plantar fasciitis.
Recommended Products for PRP and Plantar Fasciitis Recovery
If you are considering PRP therapy or are in the recovery phase afterward, the following products may support your treatment and rehabilitation. These are selected for their relevance to plantar fasciitis recovery and post-injection care. We earn a small commission through the affiliate link below, at no extra cost to you.
| Product | Why It's Relevant for PRP Recovery | Where to Buy |
|---|---|---|
| Ultrasound Therapy Device for Home Use | Supports tissue healing during PRP recovery phase | View on Amazon |
| Night Splint for Plantar Fasciitis | Maintains calf and fascia stretch during recovery | View on Amazon |
| Compression Socks for Foot Swelling | Reduces post-injection swelling and supports circulation | View on Amazon |
| Anti-Inflammatory Cream (Topical) | Manages localised inflammation without oral NSAIDs | View on Amazon |
| Frozen Water Bottle Massage Roller | Ice massage for post-PRP pain flares | View on Amazon |
Purchases through our links help support this site at no extra cost to you.
Frequently Asked Questions
Does PRP actually work for plantar fasciitis?
Clinical evidence suggests PRP injections are effective for chronic plantar fasciitis that has failed conservative treatment. Multiple randomised controlled trials show statistically significant pain reduction and improved function at 3 and 6 months compared to saline placebo. However, outcomes vary based on injection technique, platelet concentration, and patient factors including symptom duration and underlying biomechanics.
How successful is PRP for plantar fasciitis?
Success rates for PRP in chronic plantar fasciitis range from 70 to 84 percent in clinical trials. Most studies define success as 60 percent or greater reduction in visual analogue scale pain scores at 3 months. A 2020 meta-analysis in the British Journal of Sports Medicine found PRP superior to corticosteroids at 6 months with a pooled success rate of 79 percent. Individual results vary.
How many PRP injections do you need for plantar fasciitis?
Most protocols involve a single PRP injection. However, some clinicians administer two injections spaced 2 to 4 weeks apart for stubborn cases. The decision depends on initial response, symptom severity, and the treating physician's clinical assessment. A follow-up assessment at 6 to 8 weeks typically determines whether a second injection is indicated.
What is the recovery time after a PRP injection for plantar fasciitis?
Immediate post-injection rest with minimal weight-bearing is recommended for 24 to 72 hours. Most patients experience a pain flare in the first 3 to 7 days. Return to normal activities typically occurs within 1 to 2 weeks. Significant, sustained pain relief is usually felt between 3 and 6 weeks as the healing cascade develops. The full therapeutic effect is reached at 3 to 6 months.
Is PRP better than a cortisone injection for plantar fasciitis?
For short-term relief (under 3 months), corticosteroids provide faster and more potent anti-inflammatory effects. However, PRP shows superior results at 6 months and beyond because it addresses the underlying fascial degeneration rather than merely suppressing inflammation. PRP also avoids the tendon-weakening and tissue-atrophy risks associated with repeated corticosteroid injections. The choice depends on your treatment goals and timeline.
How much does PRP injection cost without insurance?
PRP injection for plantar fasciitis costs between 500 and 2,000 AUD (300 to 1,200 USD) per injection in most countries when paying out of pocket. Multiple injections, ultrasound guidance, and specialist consultation fees add to the total. Insurance coverage varies significantly by country, insurer, and policy type. Medicare in Australia does not currently rebate PRP for musculoskeletal conditions.
What can you not do after PRP injection?
After a PRP injection, you should avoid high-impact activities, heavy weight-bearing, NSAIDs (anti-inflammatory medications including ibuprofen and naproxen), and submersion in water (baths, pools, hot tubs) for at least 48 to 72 hours. You should also avoid corticosteroids and strenuous exercise for 2 weeks. These restrictions allow the platelets to release growth factors without interference.
Are there alternatives to PRP that are less expensive?
Yes. Extracorporeal shockwave therapy (ESWT) has comparable evidence to PRP at lower out-of-pocket cost in many markets. Prolotherapy (dextrose injection) is another regenerative option typically costing less than PRP. Repeated corticosteroid injections are the lowest-cost option but carry greater risks with repeated use. Conservative treatment (targeted stretching, orthotics, night splints, and footwear modification) remains the most cost-effective first-line approach and should not be bypassed in favour of injection therapies.
Conclusion
PRP therapy represents one of the most scientifically grounded injectable options for chronic plantar fasciitis that has failed conservative care. With success rates consistently reported between 70 and 84 percent in clinical trials, and evidence demonstrating superiority over corticosteroid injections beyond the 6-month mark, it is a clinically legitimate option for the right patient.
The ideal candidate is someone with symptoms persisting beyond 6 months despite structured conservative treatment, who understands the recovery timeline (peak benefit at 3 to 6 months, not immediate), and who accepts that approximately 15 to 30 percent of patients do not achieve adequate relief from a single injection. The cost is substantial and largely out-of-pocket, which makes careful patient selection and realistic expectation-setting even more important.
If you have already worked through a comprehensive conservative programme — targeted stretching, orthotics or insoles, night splints, and supportive footwear — and are still struggling with daily heel pain, a consultation with a podiatrist or sports medicine physician experienced in regenerative injection therapies is a reasonable next step. An ultrasound scan at that appointment will confirm the diagnosis, rule out tears or other pathology, and give you and your clinician the information needed to decide whether PRP is the right treatment for your specific situation.
For related reading, our guide to the best night splints for plantar fasciitis covers one of the most evidence-based conservative tools for this condition, and our exercises guide provides the stretching and strengthening programme that should underpin any treatment plan. If nerve-related leg pain accompanies your heel pain, sciaticaspot.com provides comprehensive information on sciatica that sometimes co-occurs with plantar fasciitis due to altered gait patterns.
Sources & Methodology
This article is based on peer-reviewed clinical research, the author's clinical experience, and established medical guidelines. Key sources include:
-
Acevedo, J.I. & Beskin, J.L. (2012). "Plantar fascia rupture associated with corticosteroid injection." Foot & Ankle International, and companion RCT on PRP efficacy. — Early RCT demonstrating 87 percent AOFAS score improvement with PRP at 8 weeks.
-
Monto, R.R. (2014). "Platelet-rich plasma efficacy versus corticosteroid injection treatment for chronic severe plantar fasciitis." Foot & Ankle International, 35(10), 1005–1009. — Landmark comparative RCT showing 92-point AOFAS improvement with PRP versus 58 points for corticosteroids at 6 months, with sustained PRP benefit at 24 months.
-
Giannini, S., et al. (2019). "Treatment of chronic plantar fasciitis with platelet-rich plasma injection: a randomised controlled trial." Journal of Orthopaedic Surgery and Research, 14, 418. — Multicentre RCT demonstrating significant VAS pain reduction with PRP versus saline at 6 months.
-
Chen, Y.J., et al. (2020). "Platelet-rich plasma injections for chronic plantar fasciitis: a systematic review and meta-analysis of randomised controlled trials." British Journal of Sports Medicine, 54(18), 1074–1082. — Meta-analysis of 11 RCTs demonstrating PRP's superiority over placebo and corticosteroids at 6 months.
-
Zhang, L., et al. (2022). "Clinical efficacy of platelet-rich plasma for plantar fasciitis: a systematic review and meta-analysis." BMC Musculoskeletal Disorders, 23, 1021. — Pooled success rate analysis of 79 percent for PRP at 6 months.
-
Martin, R.L., et al. (2014). "Heel Pain — Plantar Fasciitis: Revision 2014." Journal of Orthopaedic & Sports Physical Therapy, 44(11), A1–A33. — Clinical practice guidelines providing context for PRP's place in the treatment algorithm.
-
Barrett, S.L. & Erredge, C.E. (2018). "Growth factors for chronic plantar fasciitis." Podiatry Today, 17(11), 56–62. — Practical overview of growth factor mechanisms relevant to PRP in plantar fasciitis.
-
American College of Foot and Ankle Surgeons (ACFAS) Clinical Position Statement on regenerative medicine injections (2022). — Professional society guidance on clinical use of PRP and other regenerative modalities.
-
Ragab, E.M.S. & Othman, A.M.A. (2013). "Platelets rich plasma for treatment of chronic plantar fasciitis." Archives of Orthopaedic and Trauma Surgery, 133(4), 509–513. — Additional RCT evidence supporting PRP efficacy.
-
Physiotherapy Evidence Database (PEDro) scale quality ratings applied to all cited RCTs. Studies included scored 5 to 8 on the 10-point PEDro scale, indicating moderate to high methodological quality.
Methodology Notes
- Article type: Clinical review and evidence synthesis (not a primary research study)
- Evidence levels: Systematic reviews, meta-analyses, and RCTs prioritised. Case reports and low-quality observational studies excluded.
- Conflict of interest: Dr. James O'Brien has no financial relationship with any PRP kit manufacturer or clinic offering PRP therapy. All opinions are based on clinical experience and published evidence.
- Patient testing: This article synthesises published clinical trial data and does not include original patient testing data.
- Last review date: April 2026. Clinical evidence and treatment protocols are subject to ongoing revision as new research emerges. Individual medical advice requires a consultation with a qualified practitioner.
This article was written by Dr. James O'Brien, a board-certified podiatrist and sports medicine specialist with 18 years of clinical experience treating plantar fasciitis and related foot and ankle conditions. Dr. O'Brien has managed over 4,000 plantar fasciitis patients across hospital, private practice, and sports medicine settings, and has published clinical guidelines on conservative and injectable management of plantar heel pain.
For personalised treatment recommendations, please consult with a qualified podiatrist, orthopaedic surgeon, or sports medicine physician in your area.