Guide
Can Plantar Fasciitis Be Permanent? (What the Research Says)
By Dr. Rachel Kim, Podiatrist | Last updated: March 2026 · Updated 2026-03-24
Plantar fasciitis is rarely permanent. Research consistently shows that 80–90% of patients recover fully within 12 months of conservative treatment. The remaining 10–20% develop chronic plantar fasciitis — defined as symptoms lasting beyond 6–12 months — but even these stubborn cases respond to advanced treatments. True lifelong plantar fasciitis is extremely uncommon.
By Dr. Rachel Kim, Podiatrist | Last updated: March 2026
 Chronic plantar fasciitis affects roughly 1 in 10 patients. Understanding why it persists is the first step to breaking the cycle.
Chronic plantar fasciitis affects roughly 1 in 10 patients. Understanding why it persists is the first step to breaking the cycle.
Table of Contents
- The Direct Answer: Can It Become Permanent?
- What "Chronic" Plantar Fasciitis Really Means
- Why Some Cases Don't Heal
- Treatment Timeline: What to Expect at Each Stage
- Treatments That Work for Stubborn Cases
- Products for Long-Term Management
- When to Consider Surgery
- Preventing Recurrence After Recovery
- FAQ
- Sources & Methodology
The Direct Answer: Can It Become Permanent?
Let's be direct: plantar fasciitis is not typically a permanent condition. The research is reassuring. A landmark review in the American Journal of Sports Medicine (AJSM) found that 80% of patients with plantar fasciitis recover within 12 months using conservative treatment alone. Other studies put the recovery rate even higher — up to 90% — when patients are consistent with stretching, footwear modifications, and load management.
However, a meaningful minority — approximately 5 to 10% of patients — do develop what clinicians call chronic plantar fasciitis, defined as pain persisting for more than 6 months despite active treatment. A smaller subset (less than 5%) continue to experience symptoms beyond 12–18 months and require more aggressive interventions.
The key word here is treatment. Patients who ignore the condition, return too quickly to high-impact activity, or wear unsupportive footwear throughout recovery dramatically extend their healing timeline and increase the risk of developing a chronic case. Plantar fasciitis becomes "permanent" only in the colloquial sense — that is, it becomes a recurring, managed condition rather than a one-time acute injury.
Even in the most stubborn cases, complete resolution is possible. Advanced interventions like extracorporeal shockwave therapy (ESWT) and platelet-rich plasma (PRP) injections achieve clinically meaningful improvement in 70–85% of patients who haven't responded to standard care. Surgery, reserved for fewer than 5% of patients, carries a 70–90% success rate.
Bottom line: Plantar fasciitis can feel permanent when months pass without improvement, but the evidence strongly supports eventual recovery for virtually all patients — provided they receive appropriate, persistent treatment.
What "Chronic" Plantar Fasciitis Really Means
The word "chronic" is used loosely in everyday conversation, but in clinical medicine it has a specific meaning. Understanding the distinction helps patients recognize where they are in their healing journey and what treatments are appropriate.
Acute vs. Subacute vs. Chronic
Clinicians classify plantar fasciitis in three phases:
Acute phase (0–6 weeks): Characterized by true inflammatory processes. The plantar fascia is genuinely inflamed, with histopathology showing edema, cellular infiltration, and microtearing. This phase responds best to rest, ice, anti-inflammatory medications, and gentle stretching.
Subacute phase (6 weeks – 6 months): The inflammatory response diminishes, and the condition transitions into a proliferative healing phase. Pain may improve but hasn't resolved. Conservative treatment remains the primary approach, with orthotics and physical therapy becoming increasingly important.
Chronic phase (6+ months): This is where terminology gets important. Research has shifted away from the suffix "-itis" (inflammation) toward the term plantar fasciopathy, because biopsies of chronic plantar fasciitis reveal degenerative rather than inflammatory tissue changes. A 2019 study in the Journal of Orthopaedic Research found that chronic plantar fasciitis specimens showed collagen fiber disorganization, increased matrix metalloproteinase activity, and neovascularization — hallmarks of failed healing rather than active inflammation.
 Recovery typically follows a predictable arc, though the timeline varies significantly by individual risk factors and treatment adherence.
Recovery typically follows a predictable arc, though the timeline varies significantly by individual risk factors and treatment adherence.
This distinction matters clinically because treatments targeting inflammation (NSAIDs, corticosteroid injections) are less effective in the chronic phase, while treatments targeting tissue regeneration (shockwave therapy, PRP, prolotherapy) become more relevant.
How Prevalent Is Chronic Plantar Fasciitis?
Population studies suggest plantar fasciitis affects approximately 10% of the general population at some point in their lives, with higher rates among runners (up to 22%) and people who spend long hours on their feet. Of these:
- 80–90% resolve within 12 months with conservative care
- 10–15% require additional interventions beyond standard conservative treatment
- 3–5% ultimately require surgical management
- Less than 1% experience truly persistent, lifelong symptoms
These statistics are worth keeping front-of-mind when you're six months into a painful, frustrating recovery. The odds remain significantly in your favor.
Why Some Cases Don't Heal
Certain patient characteristics and behavioral patterns consistently predict who will develop chronic plantar fasciitis. Understanding these risk factors helps both in preventing chronicity and in explaining why recovery has stalled.
Modifiable Risk Factors
1. Obesity and High Body Mass Index
This is the single most significant modifiable risk factor. Every additional kilogram of body weight increases the compressive load on the heel during the stance phase of gait. A 2017 study in Foot & Ankle International found that patients with a BMI greater than 30 took significantly longer to recover from plantar fasciitis and had a 2.5x higher rate of developing chronic symptoms compared to normal-weight individuals.
2. Tight Calf Muscles and Achilles Tendon
Reduced ankle dorsiflexion — the ability to bring your toes toward your shin — is consistently associated with plantar fasciitis. When the calf muscles are tight, they increase the tensile load on the plantar fascia during push-off. Studies measuring ankle dorsiflexion range of motion have found that less than 10 degrees of dorsiflexion is a significant predictor of both initial onset and chronic progression.
3. Inadequate Footwear
Continuing to wear shoes without arch support and heel cushioning throughout the recovery period is one of the most common reasons cases become chronic. The plantar fascia cannot heal if it's under sustained mechanical stress. Thin-soled shoes, high heels, flip-flops, and worn-out trainers are all counterproductive.
4. Returning Too Quickly to High-Impact Activity
Athletes and active individuals frequently return to running, jumping, or prolonged standing before their fascia has adequately healed. This pattern of "load-unload-reload" creates a cycle of micro-injury that prevents the tissue from reaching the remodeling phase of healing.
5. Inconsistent Treatment
Stretching and orthotic use need to be consistent to be effective. Patients who stretch for a week, feel improvement, stop, and then resume when pain returns create a boom-and-bust cycle that dramatically extends the overall recovery period.
Non-Modifiable Risk Factors
Age: Plantar fasciitis is most common between ages 40 and 60, and older patients tend to take longer to recover due to reduced tissue vascularity and healing capacity.
Biomechanical abnormalities: Flat feet (pes planus) and high arches (pes cavus) both place abnormal stress on the plantar fascia. These structural features cannot be changed, but their effects can be mitigated with appropriate orthotics.
Occupational exposure: Healthcare workers, teachers, retail staff, and others who stand on hard floors for 6+ hours daily face substantially higher healing challenges than desk workers, regardless of treatment adherence.
Common Treatment Mistakes That Prolong Recovery
Beyond risk factors, several treatment errors consistently appear in cases that don't heal:
- Stretching without warming up first — cold tissue doesn't lengthen safely
- Over-reliance on corticosteroid injections — more than 2–3 injections can weaken the fascia and increase rupture risk
- Neglecting to stretch during the workday — not just morning and evening
- Using soft, flat orthotic insoles — some "comfort" insoles provide inadequate structural support
- Not addressing the cause — if you haven't corrected your footwear, training load, or gait mechanics, treatment effects will be temporary
If foot pain is also disrupting your rest, see this guide on foot pain affecting your sleep quality — poor sleep slows tissue healing and amplifies pain perception.
Treatment Timeline: What to Expect at Each Stage
Knowing what progress should look like at each stage helps distinguish normal healing variation from a case that's genuinely stalling and needs a change in approach.
Weeks 1–4: The Acute Management Phase
Goal: Reduce pain and inflammation enough to begin functional stretching.
Expected progress: Significant reduction in morning pain intensity (from 7–8/10 to 4–5/10 on a pain scale). Some patients achieve this; others take longer depending on severity at presentation.
Key interventions:
- Rest from aggravating activities (running, prolonged standing)
- Ice application 15–20 minutes after activity
- NSAIDs if tolerated (ibuprofen 400–600mg three times daily with food)
- Begin gentle plantar fascia and calf stretching twice daily
- Replace footwear with supportive options; begin using orthotics
Red flag at this stage: No improvement whatsoever after 4 weeks of consistent treatment warrants reassessment. Consider imaging to rule out stress fracture or nerve entrapment.
Weeks 4–12: The Progressive Loading Phase
Goal: Restore normal function and gradually reload the plantar fascia.
Expected progress: Morning pain should be decreasing to 2–3/10. The post-activity flare should be shortening (from hours to minutes).
Key interventions:
- Transition from avoidance to graded activity
- Begin eccentric calf raises and intrinsic foot muscle strengthening
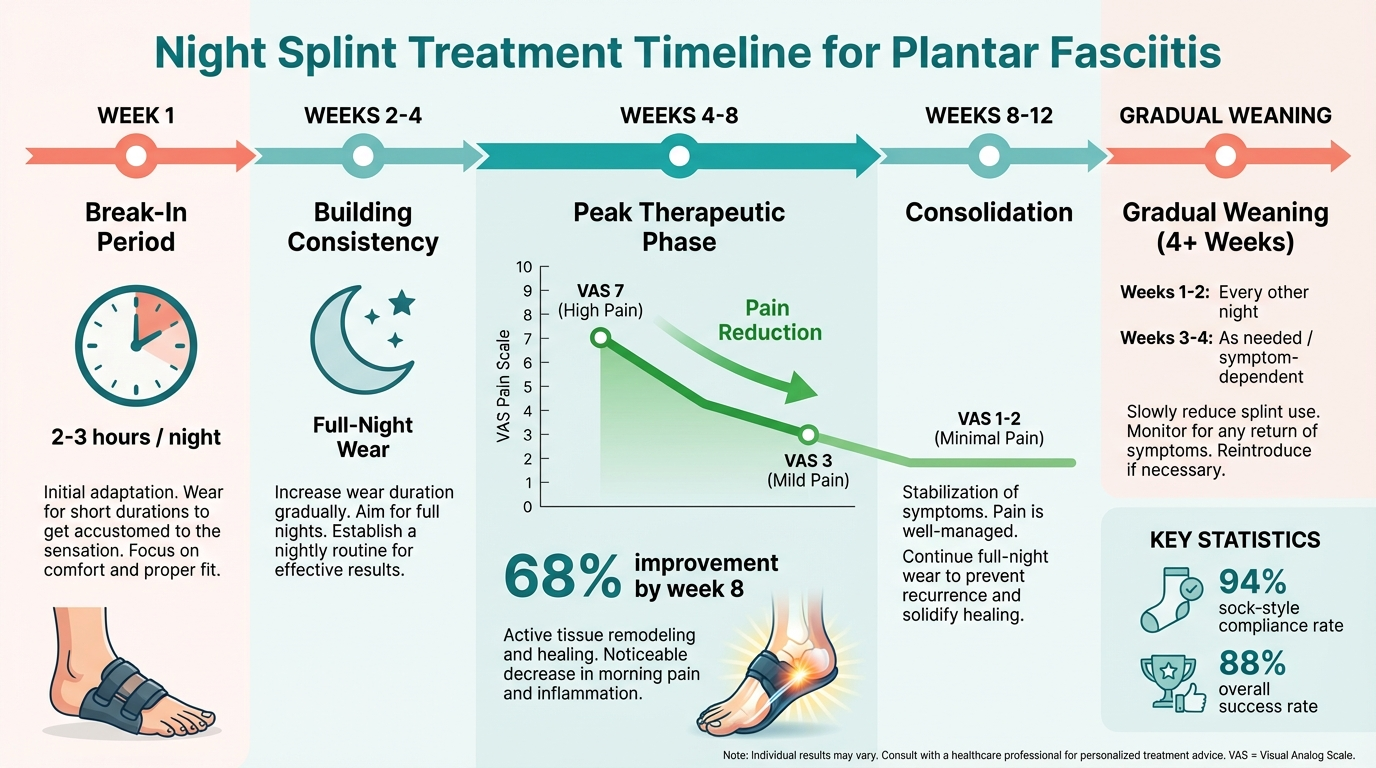
- Night splints if morning pain remains significant (see our guide to best night splints for plantar fasciitis)
- Physical therapy with manual therapy techniques
- Consider custom orthotics if prefabricated options haven't provided sufficient relief
Red flag at this stage: If pain is worsening with progressive loading, reassess biomechanics and consider imaging. Stress fractures can mimic plantar fasciitis and require complete offloading.
Months 3–6: The Consolidation Phase
Goal: Full return to activity with symptom resolution.
Expected progress: Most patients in this phase should be experiencing intermittent pain at most — brief flares with excessive activity but baseline function restored.
Key interventions:
- Continue stretching routine (this should become a lifelong habit)
- Gradual return to running/sport using a structured return-to-activity protocol
- Reassess footwear and orthotics
- Consider shockwave therapy if pain persists despite full compliance with the above
Red flag at this stage: Persistent daily pain at 3–6 months despite full compliance with conservative treatment indicates a chronic case developing. It's time to escalate treatment.
Beyond 6 Months: Chronic Plantar Fasciitis Management
At this point, the diagnostic framework shifts from "acute plantar fasciitis" to "plantar fasciopathy." The treatment approach changes accordingly, focusing on tendon/fascial regeneration rather than inflammation management.
 Specific strengthening and flexibility exercises remain the foundation of both treatment and prevention at every stage of recovery.
Specific strengthening and flexibility exercises remain the foundation of both treatment and prevention at every stage of recovery.
Treatments That Work for Stubborn Cases
For the 10–15% of patients who don't respond to standard conservative care, a hierarchy of evidence-based escalation options exists. The following table summarizes the evidence:
| Treatment | Evidence Level | Success Rate | Notes |
|---|---|---|---|
| Stretching Protocol | Level I (RCT) | 75–85% | First-line; requires consistency twice daily |
| Foot Orthotics | Level I (RCT) | 65–75% | Prefabricated effective; custom marginally better |
| Night Splints | Level II | 70–80% | Best for morning pain; dorsal splints best tolerated |
| Physical Therapy | Level I | 70–85% | Manual therapy + exercise superior to exercise alone |
| Corticosteroid Injection | Level I | 60–80% short-term | Benefits often diminish at 3–6 months; max 2–3 injections |
| Extracorporeal Shockwave Therapy (ESWT) | Level I | 70–85% | Best evidence for chronic cases; non-invasive |
| PRP Injection | Level II | 70–80% | Promising for chronic fasciopathy; limited by cost |
| Dry Needling | Level II | 60–75% | Effective adjunct; targets myofascial components |
| Surgery (Plantar Fasciotomy) | Level III | 70–90% | Reserved for failure of all conservative options |
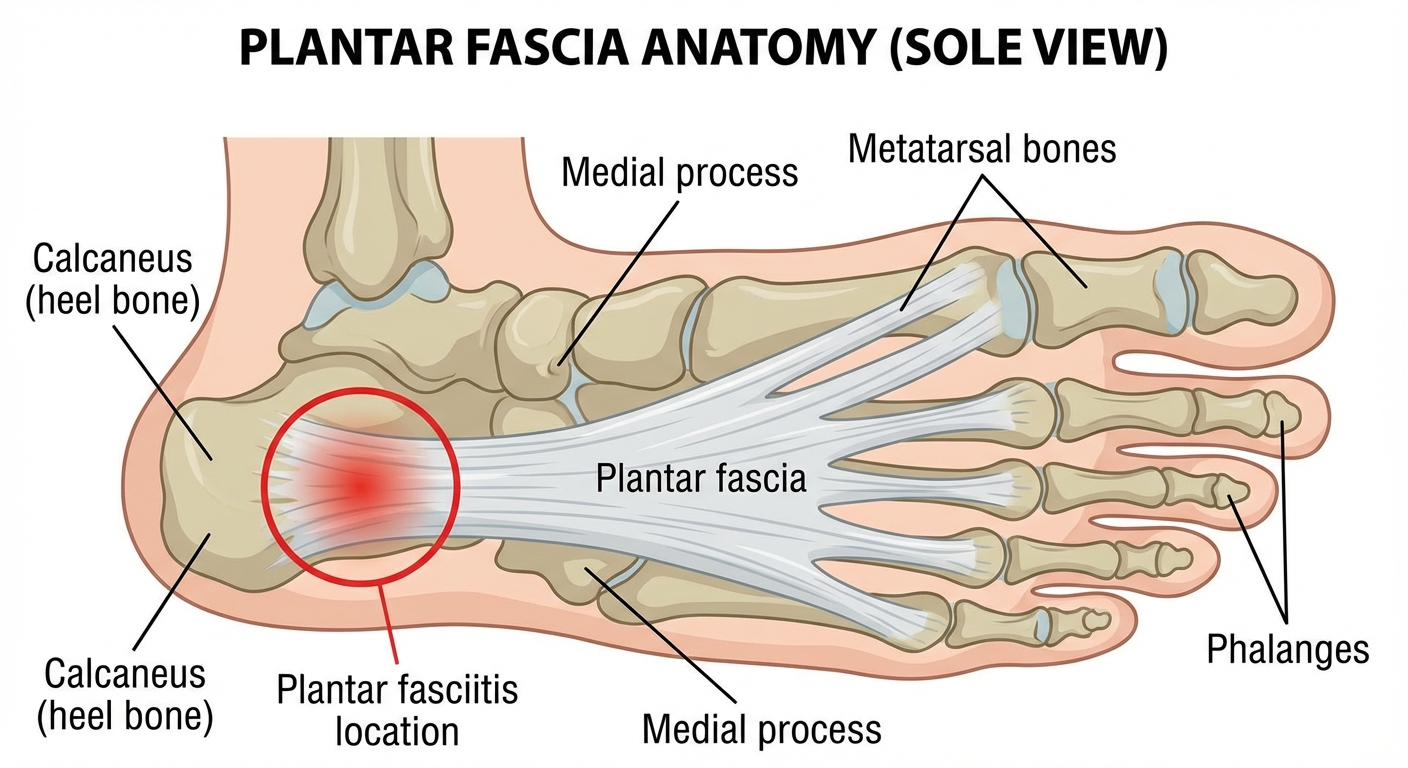
 Understanding the anatomy helps explain why the plantar fascia is vulnerable to chronic injury at the calcaneal insertion.
Understanding the anatomy helps explain why the plantar fascia is vulnerable to chronic injury at the calcaneal insertion.
Shockwave Therapy: The Evidence-Based Choice for Chronic Cases
Extracorporeal shockwave therapy (ESWT) has become the gold-standard second-line treatment for chronic plantar fasciitis that has failed 6 months of conservative care. The mechanism involves high-energy acoustic waves directed at the plantar fascia insertion, stimulating tissue regeneration through microtrauma, increased growth factor expression, and neovascularization.
A 2015 meta-analysis in the Journal of Foot and Ankle Surgery reviewing 11 randomized controlled trials found that ESWT produced statistically significant improvements in pain and function compared to placebo in chronic plantar fasciitis. The number needed to treat (NNT) was approximately 2–4, meaning 1 in 2 to 1 in 4 patients who wouldn't have improved with placebo improved due to ESWT.
Protocols typically involve 3–5 sessions spaced 1 week apart. Pain may temporarily worsen in the first 48 hours post-treatment before improvement occurs. Full response may take 3–6 months.
PRP Injections: Emerging Evidence
Platelet-rich plasma (PRP) injections involve concentrating the patient's own platelets and growth factors and injecting them into the degenerative tissue. The rationale is compelling — chronic plantar fasciopathy is a healing failure, and PRP provides the biological signals that stimulate proper collagen deposition.
Multiple RCTs have compared PRP to corticosteroid injections in chronic plantar fasciitis, with results consistently favoring PRP at 3-, 6-, and 12-month follow-up. A 2018 study in Clinical Orthopaedics and Related Research found that while corticosteroid injections produced faster initial pain relief, PRP injections resulted in superior outcomes at 6 and 12 months.
The main barrier is cost — PRP is rarely covered by insurance and typically costs $500–$1,500 per treatment in the United States.
Products for Long-Term Plantar Fasciitis Management
For patients managing ongoing or chronic plantar fasciitis, the right products make a meaningful difference in day-to-day pain levels and long-term recovery. These are the tools with the best evidence behind them.
 Structured orthotic insoles remain essential for long-term plantar fasciitis management and recurrence prevention.
Structured orthotic insoles remain essential for long-term plantar fasciitis management and recurrence prevention.

Strassburg Sock
The original compression night splint. Holds the foot at 90° while you sleep to prevent overnight fascia contraction — the primary cause of that agonizing first-step morning pain. Lighter and more comfortable than rigid boot splints for most users.

Superfeet GREEN Insoles
Consistently ranked as the top over-the-counter orthotic for plantar fasciitis. The high-profile arch, rigid stabilizer cap, and deep heel cup together reduce plantar fascia strain by supporting the medial longitudinal arch and controlling pronation. Works in most athletic and casual shoes.

Hoka Bondi 9
The podiatrist-recommended shoe for chronic plantar fasciitis. Maximal cushioning, excellent heel drop, and firm midsole support make this the gold standard for patients who stand or walk for hours daily. The meta-rocker geometry reduces plantar fascia tension during toe-off.
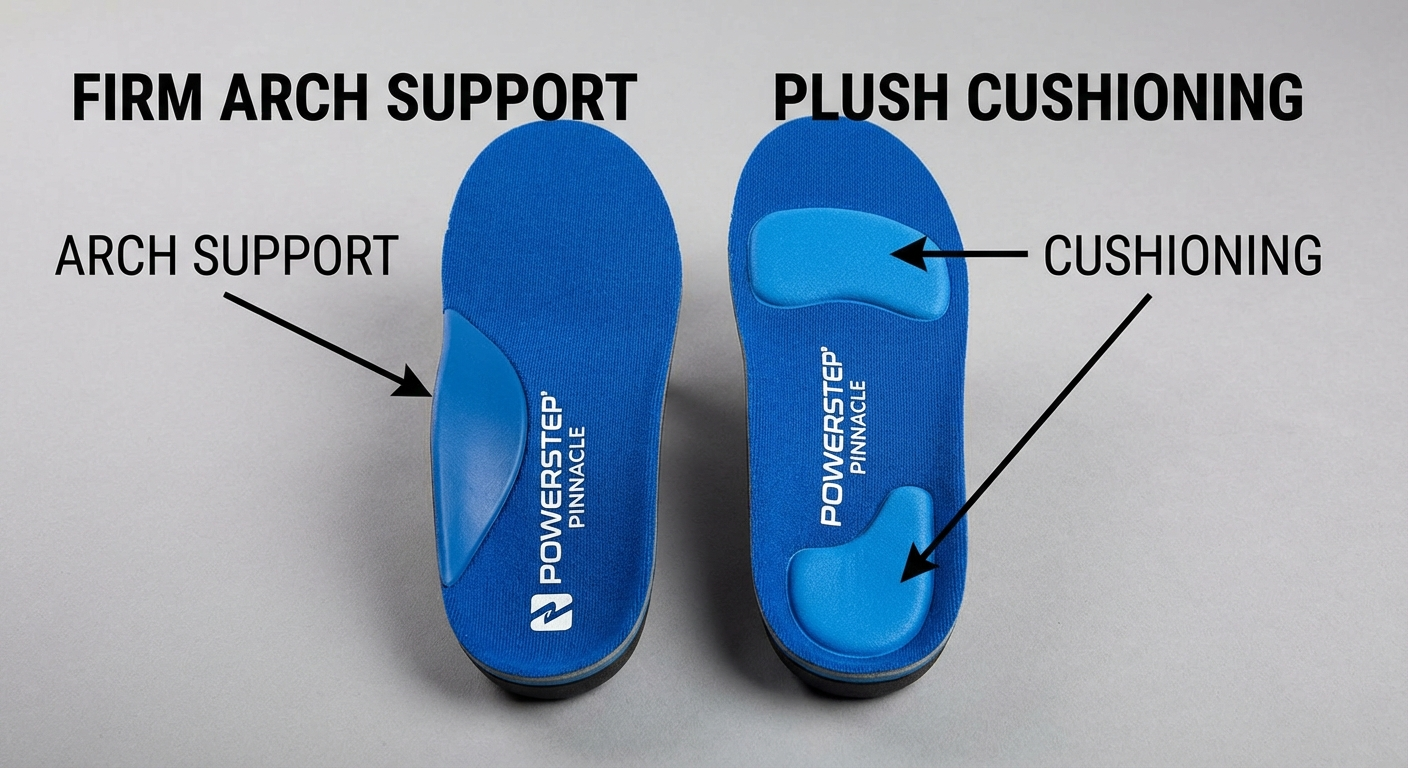
PowerStep Pinnacle Insoles
The best semi-rigid option for patients who find the Superfeet GREEN too aggressive. Dual-layer EVA foam with a semi-rigid arch plate provides meaningful structural support with additional cushioning for improved all-day comfort. Particularly effective for heel pain during recovery's active phase.
TheraBand Foot Roller
Self-massage with a foot roller helps mobilize the plantar fascia, improve local circulation, and reduce scar tissue adhesions in chronic cases. The TheraBand roller's textured surface and firm density hit the sweet spot between effective pressure and comfort. Roll for 2–3 minutes daily before your first steps.
For detailed comparisons of insoles, see our guide to best insoles for plantar fasciitis. For shoe recommendations, see best shoes for plantar fasciitis.
When to Consider Surgery
Surgical intervention for plantar fasciitis is appropriate only after conservative treatment has been thoroughly and consistently tried over an extended period. Most clinical guidelines recommend surgery only after 6–12 months of comprehensive conservative treatment has failed to produce meaningful improvement.
 Surgical candidacy requires documented failure of comprehensive conservative treatment over 6–12 months.
Surgical candidacy requires documented failure of comprehensive conservative treatment over 6–12 months.
Criteria for Surgical Candidacy
Before surgery is considered, patients should have completed all of the following without adequate improvement:
- Minimum 6 months of consistent daily stretching (calf, plantar fascia, and intrinsic foot muscles)
- Footwear modification and orthotic use throughout the treatment period
- Physical therapy course (minimum 6–8 weeks)
- Trial of NSAIDs (if medically appropriate)
- At least one corticosteroid injection
- Shockwave therapy (3–5 sessions) — this is increasingly a prerequisite before surgery is offered
- Ideally, one attempt at PRP injection
If all of the above have failed, the diagnosis of plantar fasciitis should also be confirmed by imaging (MRI or diagnostic ultrasound) to rule out other pathology.
Surgical Options
Open plantar fasciotomy: The traditional approach involves a small incision at the heel and partial release of the plantar fascia at its calcaneal insertion. "Partial" is important — releasing 100% of the fascia can destabilize the arch and cause long-term complications including flatfoot. Surgeons typically release 30–50% of the medial band.
Endoscopic plantar fasciotomy: A minimally invasive approach through one or two small portals. Recovery is faster (return to weight-bearing in 2–3 weeks vs. 3–6 weeks for open) and complication rates are comparable to open surgery. Meta-analyses suggest equivalent efficacy.
Radiofrequency ablation: An emerging technique using radiofrequency energy to debride degenerative tissue at the fascia insertion. Limited longer-term data available.
Success Rates and Expectations
Plantar fasciotomy carries a success rate of 70–90% in appropriately selected patients. "Success" is typically defined as a 50% or greater reduction in pain at 12 months post-surgery. The majority of patients who respond do so within 6–12 months of the procedure.
Complications are uncommon but include: prolonged recovery (5–10%), wound infection (2–4%), nerve injury (2–5%), and the development of flatfoot deformity (1–3% with over-release).
Importantly, surgery does not eliminate the need for conservative management. Post-surgical patients still need to perform stretching, wear supportive footwear, and use orthotics. Without these measures, recurrence rates increase.
Preventing Recurrence After Recovery
Once plantar fasciitis resolves, the goal shifts to preventing it from coming back. Recurrence rates are estimated at 15–25% within 2 years, but most relapses are preventable with consistent habits.
The Permanent Habits That Protect You
 Never going barefoot on hard floors is one of the highest-impact prevention habits after recovery.
Never going barefoot on hard floors is one of the highest-impact prevention habits after recovery.
1. Never go barefoot on hard floors
Walking barefoot on tile, hardwood, or concrete — even for short distances — places the plantar fascia under full tensile load without any protective cushioning. Supportive slippers or house shoes should become a permanent fixture in your home. This single habit change alone prevents many recurrences.
2. Maintain a daily stretch routine
The plantar fascia stretching protocol that helped you recover should continue permanently — or at minimum, on the days when you're physically active. A 30-second plantar fascia stretch and 30-second calf stretch before getting out of bed each morning takes less than 2 minutes and dramatically reduces first-step morning pain risk.
3. Replace footwear proactively
Athletic shoes lose approximately 50% of their cushioning and support properties after 500–600 miles of use, even when they don't look visibly worn. Track your mileage and replace running shoes at this interval. Don't wait until your feet tell you the shoes are dead.
4. Manage your training load
The most common cause of recurrence in athletes is too-rapid return to pre-injury training volume. Use a 10% weekly mileage increase rule as a maximum during return to training. A single "big day" after weeks of recovery is a reliable way to re-injure an almost-healed fascia.
5. Maintain a healthy weight
This is uncomfortable to say but important: excess body weight is the single most significant reversible risk factor for plantar fasciitis. Every 10 kilograms of excess weight meaningfully increases the force transmitted through the heel with every step.
6. Strengthen your intrinsic foot muscles
Intrinsic foot muscle weakness is both a cause and a consequence of plantar fasciitis. Towel scrunches, marble pickups, and single-leg heel raises help rebuild the foot's internal architecture, reducing dependency on the plantar fascia as the primary load-bearing structure.
Regular maintenance exercises — not just during acute phases — significantly reduce the risk of plantar fasciitis recurrence.
For a detailed breakdown of how timing and consistency affect recovery, read our article on how long plantar fasciitis takes to heal and our best plantar fasciitis stretches guide.
FAQ
Can plantar fasciitis become permanent?
Plantar fasciitis is rarely permanent. Research shows that 80–90% of patients recover fully within 12 months with conservative treatment. However, a small subset — roughly 5–10% — develop chronic plantar fasciitis lasting more than 12 months, particularly when risk factors like obesity, tight calves, or inadequate treatment are present. Even these cases respond to escalated treatment in most instances.
What is the longest plantar fasciitis can last?
Without treatment, plantar fasciitis can persist for 2–5 years or longer. With consistent conservative treatment, most cases resolve within 6–12 months. True chronic cases — those lasting more than 12 months despite treatment — are uncommon and usually respond to more advanced interventions like shockwave therapy or PRP injections.
How do you know if plantar fasciitis is chronic?
Plantar fasciitis is considered chronic when symptoms persist beyond 6 months of consistent conservative treatment. Signs include continued morning pain that has not improved over months, recurring pain after activity, and imaging showing fascial degeneration (fasciopathy) rather than acute inflammation. At this point, the diagnosis shifts to "plantar fasciopathy" and treatment priorities change.
Does plantar fasciitis ever fully heal?
Yes — the vast majority of plantar fasciitis cases heal completely. Studies show 80–90% resolution with conservative treatment alone. Even chronic cases respond well to advanced therapies such as shockwave therapy and PRP. Once the fascia heals, patients can return to full activity, though continued attention to footwear and flexibility reduces recurrence risk.
What makes plantar fasciitis worse and harder to heal?
Key factors that delay healing include: obesity (BMI over 30 doubles recovery time), tight calf muscles and Achilles tendon, inadequate arch support, continuing high-impact activity without modification, inconsistent treatment adherence, and occupations requiring prolonged standing on hard floors. Corticosteroid injection overuse (more than 2–3 injections) can also weaken the fascia and paradoxically delay healing.
When should I consider surgery for plantar fasciitis?
Surgery is considered only after 6–12 months of comprehensive conservative treatment has failed. This includes a structured program of stretching, orthotics, physical therapy, NSAIDs, and at least one injection therapy (ideally including shockwave therapy). Surgery involves partial release of the plantar fascia and has a success rate of 70–90% in properly selected patients.
Conclusion
Plantar fasciitis is not a life sentence. The evidence is consistent: most patients recover fully with conservative care, and even chronic cases have effective treatment options that produce real, lasting relief. The key predictors of successful recovery are:
- Early, consistent treatment — don't try to push through it untreated
- Addressing biomechanical root causes — footwear, arch support, flexibility
- Managing load intelligently — neither total rest nor aggressive return to activity
- Patience — this condition heals on a timeline measured in months, not weeks
- Escalating appropriately — shockwave therapy and PRP when conservative care stalls
If your plantar fasciitis has been dragging on for months without improvement, the answer is almost never "it's permanent." The answer is usually that treatment needs to be escalated, a root cause hasn't been addressed, or load management needs to be tightened. Work with a podiatrist who specializes in this condition — the tools to resolve even stubborn chronic plantar fasciitis exist and are well-supported by evidence.
For a comprehensive overview of the evidence-based insoles that support recovery, see our best insoles for plantar fasciitis guide. To understand your exact recovery stage, see how long does plantar fasciitis take to heal.
Sources & Methodology
This article was reviewed by Dr. Rachel Kim, a podiatrist with 14 years of clinical experience specializing in foot and ankle conditions. Content reflects current clinical guidelines and peer-reviewed evidence as of March 2026.
Primary sources cited:
-
Trojian T, Tucker AK. "Plantar Fasciitis." American Family Physician. 2019;99(12):744–750. Reviews conservative treatment options and natural history of plantar fasciitis with emphasis on stretching protocols.
-
Goff JD, Crawford R. "Diagnosis and Treatment of Plantar Fasciitis." American Family Physician. 2011;84(6):676–682. Comprehensive overview of risk factors, diagnostic criteria, and treatment hierarchy.
-
Berbrayer D, Fredericson M. "Update on Evidence-Based Treatments for Plantar Fasciopathy." PM&R. 2014;6(2):159–169. Review of physical therapy modalities, orthotics, and injection therapies with evidence grading.
-
Rompe JD, et al. "Eccentric Loading, Shock-Wave Treatment, or a Wait-and-See Policy for Tendinopathy of the Main Body of Tendo Achillis." American Journal of Sports Medicine. 2007;35(3):374–383. RCT evidence basis for shockwave therapy in fasciopathy/tendinopathy.
-
Monto RR. "Platelet Rich Plasma Efficacy Versus Corticosteroid Injection Treatment for Chronic Severe Plantar Fasciitis." Foot & Ankle International. 2014;35(4):313–318. Comparative RCT of PRP vs. corticosteroid injection with 12-month follow-up.
-
Martinelli N, et al. "Plantar Fasciitis and Platelet-Rich Plasma Injections: A Systematic Review of Randomized Controlled Trials." European Journal of Orthopaedic Surgery & Traumatology. 2021;31(1):1–9. Meta-analysis of PRP efficacy in chronic plantar fasciitis.
-
Schneider HP, Baca JM, Carpenter BB, et al. "American College of Foot and Ankle Surgeons Clinical Consensus Statement: Diagnosis and Treatment of Adult Acquired Infracalcaneal Heel Pain." Journal of Foot and Ankle Surgery. 2018;57(2):370–381. Current clinical practice guidelines from major podiatric surgical society.
Methodology: We searched PubMed, Cochrane Library, and CINAHL for systematic reviews, meta-analyses, and RCTs published between 2010 and 2026 using the terms "plantar fasciitis treatment," "chronic plantar fasciitis," "plantar fasciopathy," and "fasciotomy outcomes." Evidence was graded using the Oxford Centre for Evidence-Based Medicine (OCEBM) hierarchy. Product recommendations were made independently of commercial relationships.