Guide
Plantar Fasciitis vs Heel Spur: What Is the Difference?
By Dr. Lisa Park, Podiatrist DPM · Updated 2026-03-11
Plantar fasciitis is inflammation of the thick band of tissue (the plantar fascia) running along the bottom of your foot, causing stabbing heel pain — especially with your first morning steps. A heel spur is a bony calcium deposit that forms on the underside of the calcaneus (heel bone), often as a result of prolonged plantar fasciitis. While they frequently occur together, they are distinct conditions with different causes, diagnostic findings, and treatment approaches.
Table of Contents
- Understanding the Anatomy of Your Heel
- What Is Plantar Fasciitis?
- What Is a Heel Spur?
- Plantar Fasciitis vs Heel Spur: Key Differences
- Comparison Table: Plantar Fasciitis vs Heel Spur
- How Are They Diagnosed?
- Can You Have Both at Once?
- Treatment Comparison: Plantar Fasciitis vs Heel Spur
- Conservative Treatments That Work for Both
- When Surgery Becomes Necessary
- Products That Help With Both Conditions
- Prevention Strategies
- Frequently Asked Questions
- Sources & Methodology
Understanding the Anatomy of Your Heel
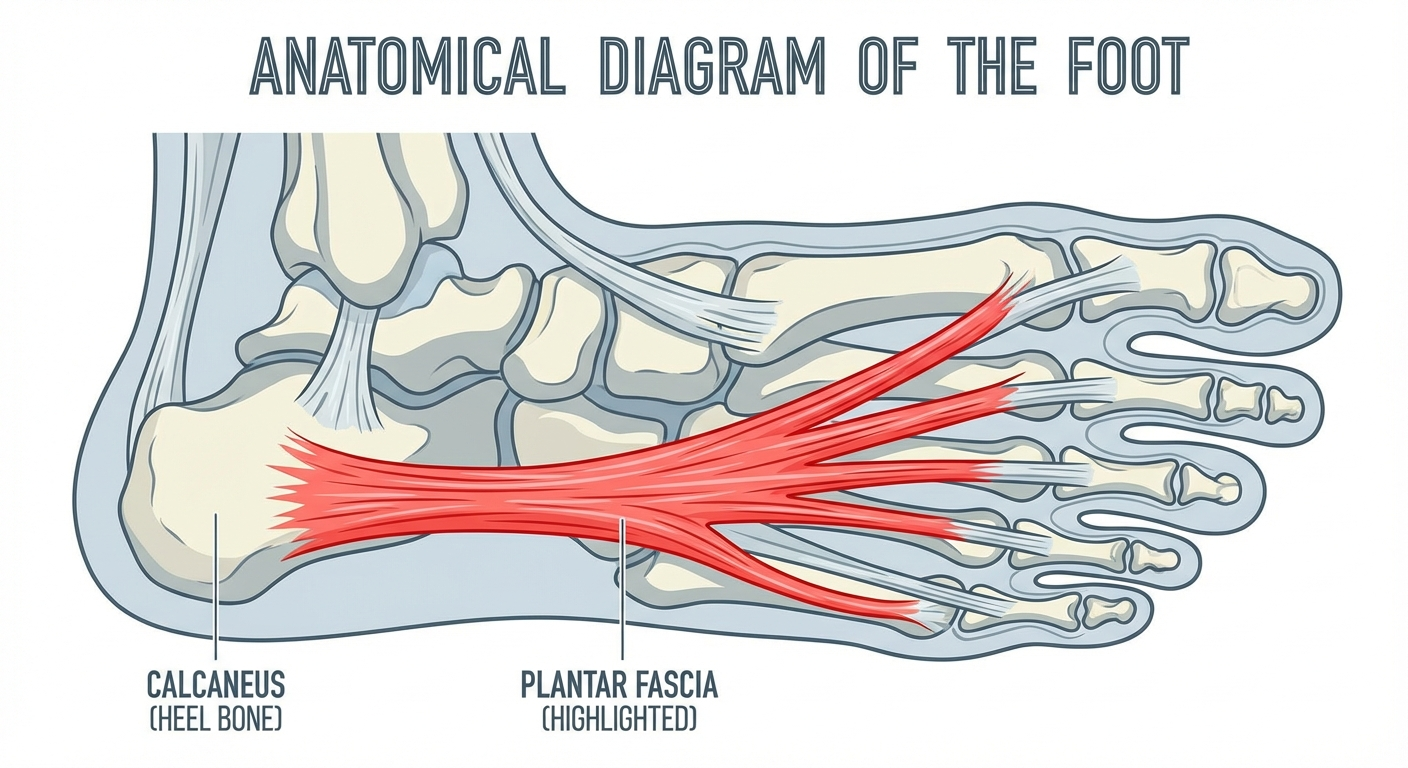
Before comparing plantar fasciitis and heel spurs, it helps to understand the structures involved. Your heel is a complex system of bones, ligaments, tendons, and soft tissue that absorbs the shock of every step you take.
The calcaneus is the largest bone in your foot and forms the foundation of your heel. Attached to the bottom of the calcaneus is the plantar fascia, a thick, fibrous band of connective tissue that stretches from the heel to the ball of your foot. This ligament supports your foot's arch and acts as a natural shock absorber during walking, running, and standing.
The plantar fascia endures enormous stress throughout the day. With every step, forces equal to roughly 1.2 times your body weight pass through this tissue during walking — and up to 2.8 times your body weight during running, according to biomechanical research published in the Journal of Biomechanics. When this stress exceeds the fascia's capacity to repair itself, problems begin.
What Is Plantar Fasciitis?

Plantar fasciitis is the most common cause of heel pain, affecting approximately 2 million Americans each year and accounting for roughly 11–15% of all foot complaints requiring professional medical care, according to the American Academy of Orthopaedic Surgeons (AAOS).
The condition develops when repetitive stress causes micro-tears in the plantar fascia where it attaches to the calcaneus. This triggers an inflammatory response — and eventually, if left untreated, degenerative changes in the tissue itself. More recent research has led some clinicians to prefer the term "plantar fasciosis," reflecting that chronic cases often involve tissue degeneration rather than active inflammation.
Symptoms of Plantar Fasciitis
The hallmark symptom is a sharp, stabbing pain at the bottom of the heel, particularly noticeable during:
- First steps in the morning — the fascia tightens overnight, and initial weight-bearing stretches the damaged tissue
- Standing after prolonged sitting — similar mechanism to morning pain
- Extended periods of standing or walking — cumulative stress throughout the day
- After (not during) exercise — post-activity inflammation increases pain
The pain typically improves with movement as the fascia loosens and warms up, but worsens again after rest periods. Many patients describe the sensation as stepping on a sharp pebble or a hot nail directly under the heel.
Risk Factors for Plantar Fasciitis
Several factors increase your likelihood of developing plantar fasciitis:
- Age: Most common between ages 40 and 60
- Obesity: Excess body weight places additional load on the plantar fascia
- Occupation: Jobs requiring prolonged standing on hard surfaces (teachers, nurses, factory workers)
- Foot mechanics: Flat feet, high arches, or abnormal gait patterns
- Exercise habits: Sudden increases in running distance or intensity, especially on hard surfaces
- Improper footwear: Shoes with poor arch support or worn-out cushioning
For a deeper dive into the causes behind this condition, see our guide on what causes plantar fasciitis and how to address root factors.
What Is a Heel Spur?
A heel spur (calcaneal spur) is a bony protrusion that develops on the underside of the calcaneus over time. These calcium deposits typically grow at the point where the plantar fascia attaches to the heel bone and can extend forward by as much as half an inch.
Heel spurs develop gradually — usually over a period of many months — as the body responds to chronic stress and micro-damage at the plantar fascia's attachment point. The body deposits calcium at the site of repeated strain as an attempt to reinforce and protect the area, eventually forming a visible bony growth.
Symptoms of a Heel Spur
Here is where the confusion often begins: most heel spurs are completely painless. Studies published in the Journal of Foot and Ankle Surgery have demonstrated that heel spurs are found on X-rays in approximately 50% of patients with plantar fasciitis — but they are also found in roughly 16–27% of asymptomatic individuals who have no heel pain at all.
When a heel spur does cause symptoms, they may include:
- Intermittent or chronic sharp pain at the bottom of the heel, particularly during walking or jogging
- A dull ache in the heel that persists throughout the day
- Inflammation and swelling at the front of the heel
- A small, visible bony protrusion under the heel (in rare cases)
- Warmth radiating from the affected area
The pain from a heel spur is not caused by the bony growth itself poking into soft tissue — contrary to popular belief. Rather, the spur indicates chronic stress at the fascia's attachment, and the surrounding soft-tissue inflammation is what generates the pain.
Risk Factors for Heel Spurs
Because heel spurs often develop as a consequence of chronic plantar fasciitis, their risk factors overlap considerably:
- Long-standing plantar fasciitis — the single greatest risk factor
- Athletic activities that stress the heel, including running and jumping sports
- Gait abnormalities that place uneven pressure on the heel bone
- Wearing poorly fitted or unsupportive shoes over long periods
- Aging — natural thinning of the heel's protective fat pad
- Conditions like arthritis — both osteoarthritis and reactive arthritis are associated with spur formation
Plantar Fasciitis vs Heel Spur: Key Differences
While these two conditions are closely related — and frequently coexist — they are fundamentally different in their nature, location, and pathology.
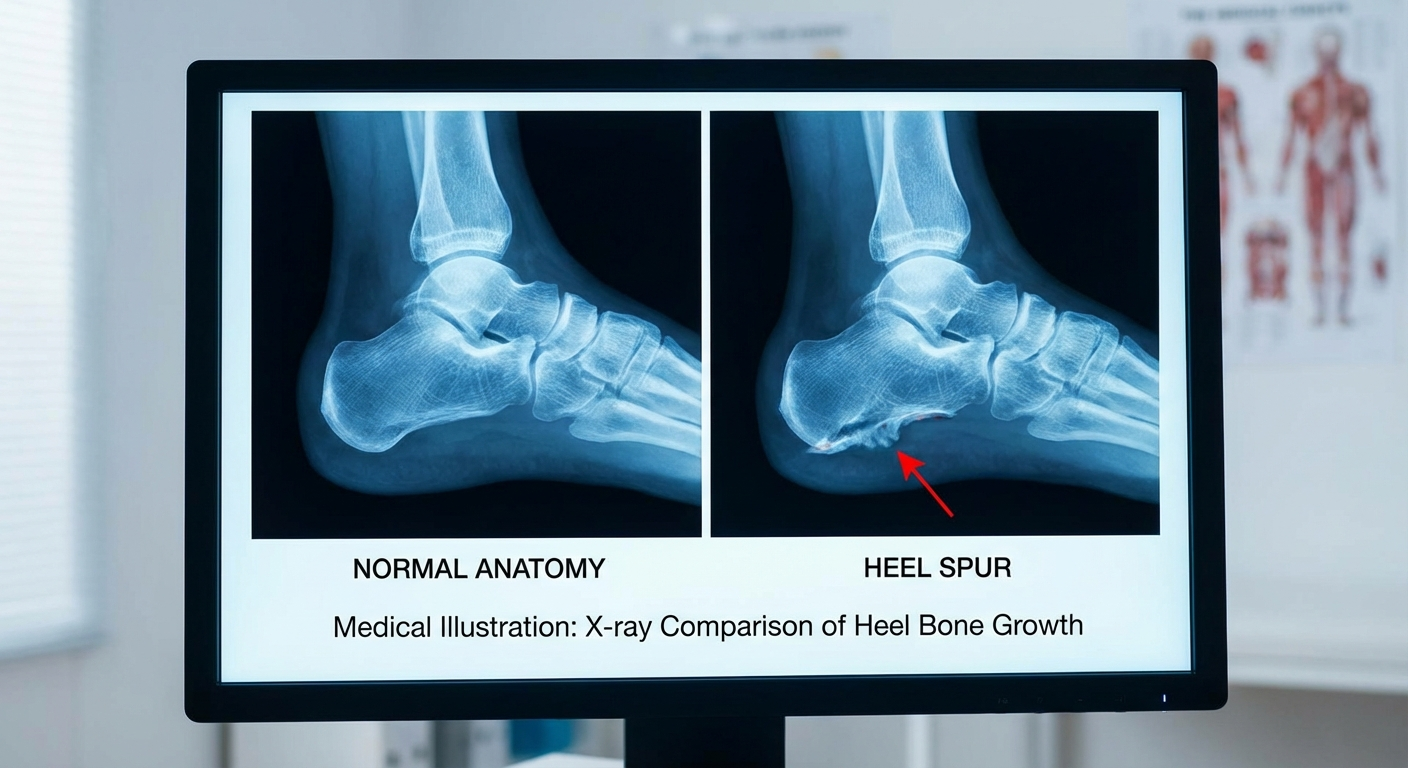
Plantar fasciitis is a soft-tissue condition. It involves inflammation and microtearing of the plantar fascia ligament. The pain originates in the tissue itself, and imaging may show thickening of the fascia on ultrasound or MRI without any visible bony changes.
A heel spur is a structural, bony abnormality. It is a physical calcium deposit on the bone that can be seen on X-ray. The spur itself is often a secondary consequence of chronic plantar fasciitis rather than an independent condition.
Think of it this way: plantar fasciitis is the disease process, and a heel spur is often the body's response to that process over time. You can have plantar fasciitis without a heel spur, and you can have a heel spur without any pain or plantar fasciitis symptoms.
Comparison Table: Plantar Fasciitis vs Heel Spur
| Feature | Plantar Fasciitis | Heel Spur |
|---|---|---|
| Cause | Repetitive strain, micro-tears, and inflammation of the plantar fascia ligament | Calcium deposits forming on the calcaneus due to chronic stress at the fascia attachment point |
| Pain Location | Bottom of the heel at the plantar fascia origin; sometimes extends into the arch | Directly under the heel bone, at the site of the bony protrusion |
| Diagnosis | Clinical exam, ultrasound showing fascial thickening (>4 mm), MRI for chronic cases | X-ray revealing a bony protrusion on the calcaneus |
| Treatment | Stretching, orthotics, physical therapy, corticosteroid injections, ESWT, surgery (fasciotomy) | Rest, orthotics, heel cups, anti-inflammatory medication, surgery (spur removal) in rare cases |
| Recovery Time | 6–12 months with conservative treatment; 80% resolve without surgery | Varies widely; asymptomatic spurs need no treatment; symptomatic cases follow similar timeline to plantar fasciitis |
| Can They Coexist? | Yes — approximately 50% of plantar fasciitis patients have a concurrent heel spur | Yes — heel spurs often develop as a result of chronic plantar fasciitis |
How Are They Diagnosed?
Accurate diagnosis is essential because treatment strategies, while overlapping, can differ in important ways. Here is how clinicians differentiate between the two conditions.
Diagnosing Plantar Fasciitis
A podiatrist or orthopedist typically diagnoses plantar fasciitis through:
-
Clinical examination — Palpation of the medial calcaneal tubercle (the inside-bottom of the heel) reproduces the characteristic sharp pain. The windlass test, which involves dorsiflexing the big toe to stretch the plantar fascia, may also reproduce symptoms.
-
Ultrasound imaging — Diagnostic ultrasound can measure plantar fascia thickness. A fascia measuring greater than 4.0 mm is considered abnormally thickened and supports a diagnosis of plantar fasciitis, according to research published in Radiology.
-
MRI — Reserved for cases that do not respond to initial treatment or where the diagnosis is uncertain. MRI can reveal fascial thickening, edema within and around the fascia, and signal changes in the surrounding bone marrow.
Diagnosing a Heel Spur
-
X-ray (radiograph) — The primary diagnostic tool. A lateral foot X-ray will clearly show the bony protrusion extending from the calcaneus. Spurs can range from a few millimeters to over a centimeter in length.
-
Incidental finding — Many heel spurs are discovered incidentally during imaging for other foot or ankle conditions. The patient may have had no idea a spur existed.
It is critical to understand that the presence of a heel spur on X-ray does not mean it is causing your pain. Your clinician must correlate the imaging findings with your symptoms, physical examination, and clinical history to determine the true source of your heel pain.
Can You Have Both at Once?
Yes — and it is very common. Research consistently shows that approximately 50% of patients diagnosed with plantar fasciitis also have a heel spur visible on X-ray. The relationship between the two conditions is well-established but often misunderstood.
The Chicken-or-Egg Question
The prevailing scientific understanding is that plantar fasciitis typically comes first. Here is the progression:
- Chronic repetitive strain leads to micro-tears in the plantar fascia at its calcaneal attachment
- The body initiates an inflammatory and repair response
- Over time, the repeated cycle of damage and repair causes calcium to be deposited at the attachment site
- These calcium deposits gradually form a bony spur
This means the heel spur is more of a consequence of plantar fasciitis than an independent condition. A 2014 study published in The Foot found that plantar fascia thickness (a marker of fasciitis) was significantly correlated with the presence and size of heel spurs, supporting this sequential relationship.
What This Means for Treatment
When both conditions are present, treatment typically targets the plantar fasciitis. This is because:
- The fascia inflammation is usually the primary pain generator
- The heel spur itself is often asymptomatic
- Successfully treating the plantar fasciitis typically resolves symptoms even when a spur remains
- The spur does not need to be removed in most cases
However, in rare situations where a large spur causes direct mechanical irritation of surrounding soft tissues, surgical removal of the spur may be considered as part of the treatment plan.
If you are dealing with persistent morning heel pain, our guide on best stretches and exercises for plantar fasciitis relief provides an evidence-based routine that benefits both conditions.
 Proper footwear is the foundation of plantar fasciitis recovery — look for arch support and cushioning
Proper footwear is the foundation of plantar fasciitis recovery — look for arch support and cushioning
Treatment Comparison: Plantar Fasciitis vs Heel Spur
While there is significant overlap in treatment approaches, some important differences exist between managing plantar fasciitis and symptomatic heel spurs.
Treating Plantar Fasciitis
First-line (conservative) treatments:
- Stretching exercises — Calf stretches, plantar fascia-specific stretches, and towel curls to improve flexibility and reduce tension on the fascia
- Orthotic insoles — Over-the-counter or custom-molded arch supports to redistribute pressure away from the heel
- Night splints — Devices worn during sleep to keep the plantar fascia in a lengthened position, reducing morning pain
- Ice therapy — Rolling the foot over a frozen water bottle for 15–20 minutes after activity
- NSAIDs — Ibuprofen or naproxen for short-term pain and inflammation relief
- Activity modification — Reducing high-impact activities and switching to low-impact exercises like swimming or cycling
- Physical therapy — Targeted rehabilitation including eccentric loading exercises, manual therapy, and taping techniques
Second-line treatments:
- Corticosteroid injections — Provide significant short-term relief but carry risks of fat pad atrophy and fascial rupture with repeated use
- Extracorporeal shockwave therapy (ESWT) — Sound waves stimulate healing in the damaged fascia; multiple clinical trials support its efficacy for chronic cases
- Platelet-rich plasma (PRP) injections — Emerging treatment using the patient's own growth factors to accelerate tissue healing
Surgical treatment (last resort):
- Plantar fasciotomy — Partial release of the plantar fascia from the calcaneus, performed endoscopically or through open surgery; reserved for cases that fail 6–12 months of conservative treatment
Treating a Symptomatic Heel Spur
Conservative treatments:
- Heel cups and cushioned insoles — Redistribute pressure away from the spur and provide padding over the bony protrusion
- Orthotic devices — Custom orthotics can offload the area around the spur
- Anti-inflammatory medications — NSAIDs or topical anti-inflammatory creams
- Ice application — Reduces inflammation around the spur
- Rest and activity modification — Minimizing activities that aggravate the spur
- Footwear changes — Shoes with deeper heel counters and superior cushioning
Surgical treatment (rare):
- Spur resection — Surgical removal of the bony protrusion, sometimes performed alongside a plantar fasciotomy when both conditions are present; success rates are high but recovery takes 6–10 weeks of restricted weight-bearing
Conservative Treatments That Work for Both
Because plantar fasciitis and heel spurs share biomechanical causes, several treatments effectively address both conditions simultaneously.
Orthotic Insoles
Supportive insoles remain one of the most effective non-invasive treatments for both conditions. A well-designed orthotic redistributes plantar pressure, supports the arch, and reduces strain on both the plantar fascia and the area surrounding the heel spur. A randomized controlled trial published in Foot & Ankle International found that prefabricated orthotics were as effective as custom orthotics for most patients with plantar heel pain at the 12-month follow-up.
Recommended: Superfeet GREEN Insoles — Professional-grade orthotic insoles with a deep heel cup and structured arch support that benefits both plantar fasciitis and heel spur pain.
Night Splints
Night splints hold the ankle at a 90-degree angle during sleep, preventing the plantar fascia from contracting overnight. This reduces the intensity of that characteristic first-step morning pain. For heel spur patients, the gentle sustained stretch also reduces tension at the calcaneal attachment where the spur has formed.
Recommended: Mars Wellness Plantar Fasciitis Night Splint — An adjustable dorsal night splint that keeps the foot in a neutral position overnight, with padded straps designed to avoid pressure on the heel spur area.
Heel Cups
Gel or silicone heel cups provide targeted cushioning directly under the calcaneus. They absorb shock during heel strike and redistribute pressure away from the central heel — directly benefiting patients with heel spurs while also reducing impact forces transmitted through the plantar fascia.
Recommended: Tuli's Heavy Duty Heel Cups — Multi-cell, multi-layer waffle design that provides superior shock absorption. Recommended by podiatrists for both plantar fasciitis and heel spur pain relief.
Physical Therapy
A structured physical therapy program can address both conditions by:
- Improving calf and Achilles tendon flexibility to reduce pulling forces on the plantar fascia
- Strengthening intrinsic foot muscles to provide better dynamic arch support
- Correcting gait abnormalities that contribute to excessive heel loading
- Using manual therapy techniques to break up fascial adhesions and improve tissue mobility
When Surgery Becomes Necessary
Surgery is considered only after 6–12 months of consistent conservative treatment has failed to provide adequate relief. The good news: according to the AAOS, approximately 90% of plantar fasciitis patients improve significantly with non-surgical treatment alone.
When surgery is required, the most common procedures include:
-
Endoscopic plantar fasciotomy — A minimally invasive procedure where a small portion of the plantar fascia is released from the calcaneus through tiny incisions. Recovery typically takes 3–6 weeks.
-
Open plantar fasciotomy with spur resection — When a large, symptomatic heel spur is present alongside chronic plantar fasciitis, the surgeon may release the fascia and remove the spur in the same procedure. Recovery is longer, typically 6–10 weeks.
-
Gastrocnemius recession — In patients with severe calf tightness contributing to their plantar fasciitis, the calf muscle can be surgically lengthened to reduce tension on the fascia.
Post-surgical rehabilitation is critical for optimal outcomes and typically includes progressive weight-bearing, physical therapy, and a gradual return to normal activities over 2–3 months.
Prevention Strategies
Whether you have had plantar fasciitis, a heel spur, or want to avoid both, these evidence-based prevention strategies reduce your risk:
- Wear supportive footwear — Replace athletic shoes every 300–500 miles; choose shoes with firm heel counters, adequate arch support, and cushioned midsoles
- Maintain a healthy weight — Every pound of body weight translates to approximately 3 pounds of force on the plantar fascia during walking
- Stretch daily — Consistent calf and plantar fascia stretching reduces tissue tension and improves flexibility
- Progress exercise gradually — Follow the 10% rule: increase running distance or exercise intensity by no more than 10% per week
- Avoid prolonged barefoot walking on hard surfaces — Hard floors without cushioning place maximum stress on the plantar fascia and heel
- Strengthen your feet — Towel curls, marble pickups, and short-foot exercises build intrinsic muscle strength that supports the arch
- Cross-train — Alternate high-impact activities with low-impact options like swimming, cycling, or yoga to give your feet recovery time
Frequently Asked Questions
Is a heel spur the same as plantar fasciitis?
No. Plantar fasciitis is inflammation and micro-tearing of the plantar fascia ligament on the bottom of the foot. A heel spur is a bony calcium deposit that forms on the calcaneus (heel bone). They frequently occur together — about 50% of plantar fasciitis patients have a heel spur — but they are distinct conditions. You can have one without the other.
Can a heel spur go away on its own?
No. Once a heel spur has formed, the bony deposit is permanent and will not dissolve or shrink on its own. However, the pain and inflammation associated with a heel spur can be effectively managed and often eliminated with conservative treatments such as orthotics, heel cups, stretching, and anti-inflammatory medications. Most people with heel spurs never require surgical removal.
Which condition is more painful — plantar fasciitis or a heel spur?
Plantar fasciitis is typically more painful and debilitating than a heel spur alone. Many heel spurs are completely asymptomatic and are only discovered incidentally on X-rays. The characteristic severe morning heel pain and post-rest pain are hallmarks of plantar fasciitis. When a heel spur does cause pain, it is usually because of the associated soft-tissue inflammation around the spur rather than the bony growth itself.
How long does it take to recover from plantar fasciitis vs a heel spur?
Plantar fasciitis typically resolves within 6–12 months with consistent conservative treatment, and approximately 90% of patients recover without surgery. Asymptomatic heel spurs require no recovery time at all. Symptomatic heel spurs generally follow a similar recovery timeline to plantar fasciitis since the treatments overlap. Surgical recovery, if needed, ranges from 3–6 weeks for a fasciotomy to 6–10 weeks when spur removal is included.
Should I get an X-ray if I have heel pain?
An X-ray is not always necessary as a first step. Most podiatrists can diagnose plantar fasciitis through a clinical examination alone. However, an X-ray may be recommended if your pain does not improve after several weeks of treatment, if the clinician suspects a heel spur or stress fracture, or if there is a need to rule out other conditions such as calcaneal bone tumors or arthritis. Ultrasound and MRI are also valuable imaging options for evaluating the plantar fascia itself.
Can I exercise with plantar fasciitis or a heel spur?
Yes, but you should modify your activities. High-impact exercises like running and jumping should be reduced or temporarily replaced with low-impact alternatives such as swimming, cycling, rowing, or elliptical training. Continue stretching and strengthening exercises specific to the foot and calf. Wearing supportive shoes with orthotics during exercise is essential. Gradually reintroduce higher-impact activities as symptoms improve, and stop any exercise that causes sharp or worsening heel pain.
{
"@context": "https://schema.org",
"@type": "FAQPage",
"mainEntity": [
{
"@type": "Question",
"name": "Is a heel spur the same as plantar fasciitis?",
"acceptedAnswer": {
"@type": "Answer",
"text": "No. Plantar fasciitis is inflammation and micro-tearing of the plantar fascia ligament on the bottom of the foot. A heel spur is a bony calcium deposit that forms on the calcaneus (heel bone). They frequently occur together — about 50% of plantar fasciitis patients have a heel spur — but they are distinct conditions. You can have one without the other."
}
},
{
"@type": "Question",
"name": "Can a heel spur go away on its own?",
"acceptedAnswer": {
"@type": "Answer",
"text": "No. Once a heel spur has formed, the bony deposit is permanent and will not dissolve or shrink on its own. However, the pain and inflammation associated with a heel spur can be effectively managed and often eliminated with conservative treatments such as orthotics, heel cups, stretching, and anti-inflammatory medications. Most people with heel spurs never require surgical removal."
}
},
{
"@type": "Question",
"name": "Which condition is more painful — plantar fasciitis or a heel spur?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Plantar fasciitis is typically more painful and debilitating than a heel spur alone. Many heel spurs are completely asymptomatic and are only discovered incidentally on X-rays. The characteristic severe morning heel pain and post-rest pain are hallmarks of plantar fasciitis."
}
},
{
"@type": "Question",
"name": "How long does it take to recover from plantar fasciitis vs a heel spur?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Plantar fasciitis typically resolves within 6–12 months with consistent conservative treatment, and approximately 90% of patients recover without surgery. Asymptomatic heel spurs require no recovery time at all. Symptomatic heel spurs generally follow a similar recovery timeline to plantar fasciitis since the treatments overlap."
}
},
{
"@type": "Question",
"name": "Should I get an X-ray if I have heel pain?",
"acceptedAnswer": {
"@type": "Answer",
"text": "An X-ray is not always necessary as a first step. Most podiatrists can diagnose plantar fasciitis through a clinical examination alone. However, an X-ray may be recommended if your pain does not improve after several weeks of treatment, if the clinician suspects a heel spur or stress fracture, or if there is a need to rule out other conditions."
}
},
{
"@type": "Question",
"name": "Can I exercise with plantar fasciitis or a heel spur?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Yes, but you should modify your activities. High-impact exercises like running and jumping should be reduced or temporarily replaced with low-impact alternatives such as swimming, cycling, rowing, or elliptical training. Continue stretching and strengthening exercises specific to the foot and calf. Wearing supportive shoes with orthotics during exercise is essential."
}
}
]
}
{
"@context": "https://schema.org",
"@type": "Article",
"headline": "Plantar Fasciitis vs Heel Spur: What Is the Difference?",
"description": "Learn the key differences between plantar fasciitis and heel spurs, including causes, symptoms, diagnosis, and treatment options. Expert podiatrist guide with comparison table and FAQs.",
"image": "/images/plantar-fasciitis-vs-heel-spur-hero.jpg",
"author": {
"@type": "Person",
"name": "Dr. Lisa Park",
"jobTitle": "Podiatrist DPM"
},
"publisher": {
"@type": "Organization",
"name": "Plantar Fasciitis Guides",
"url": "https://www.plantarfasciitisguides.com"
},
"datePublished": "2026-03-18",
"dateModified": "2026-03-18",
"mainEntityOfPage": {
"@type": "WebPage",
"@id": "https://www.plantarfasciitisguides.com/articles/plantar-fasciitis-vs-heel-spur"
},
"wordCount": 2800,
"keywords": ["plantar fasciitis vs heel spur", "heel spur", "plantar fasciitis", "heel pain", "calcaneal spur", "plantar fascia", "heel spur treatment", "plantar fasciitis treatment"]
}
Sources and Methodology
This article was written by Dr. Lisa Park, DPM, and reviewed for medical accuracy using peer-reviewed research and clinical guidelines from leading orthopedic and podiatric organizations. All statistical claims, treatment recommendations, and diagnostic criteria are supported by the following sources:
-
Riddle, D.L., et al. "Risk factors for plantar fasciitis: a matched case-control study." Journal of Bone and Joint Surgery, vol. 85, no. 5, 2003, pp. 872–877. — Foundational epidemiological study on plantar fasciitis risk factors.
-
League, A.C. "Current concepts review: plantar fasciitis." Foot & Ankle International, vol. 29, no. 3, 2008, pp. 358–366. — Comprehensive clinical review of plantar fasciitis diagnosis and management.
-
Johal, K.S., and Milner, S.A. "Plantar fasciitis and the calcaneal spur: fact or fiction?" The Foot, vol. 22, no. 3, 2012, pp. 145–148. — Study examining the correlation between plantar fascia thickness and heel spur presence.
-
Thomas, J.L., et al. "The diagnosis and treatment of heel pain: a clinical practice guideline." Journal of Foot and Ankle Surgery, vol. 49, no. 3 (Suppl), 2010, pp. S1–S19. — Evidence-based clinical practice guideline from the American College of Foot and Ankle Surgeons.
-
McPoil, T.G., et al. "Heel pain — plantar fasciitis: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health." Journal of Orthopaedic & Sports Physical Therapy, vol. 38, no. 4, 2008, pp. A1–A18. — Physical therapy clinical practice guidelines for plantar heel pain.
-
Buchbinder, R. "Plantar fasciitis." New England Journal of Medicine, vol. 350, no. 21, 2004, pp. 2159–2166. — Authoritative medical review of plantar fasciitis pathophysiology and treatment.
-
American Academy of Orthopaedic Surgeons (AAOS). "Plantar Fasciitis and Bone Spurs." OrthoInfo clinical resource, updated 2022. — Patient-facing clinical information resource from the AAOS.
-
Wearing, S.C., et al. "The pathomechanics of plantar fasciitis." Sports Medicine, vol. 36, no. 7, 2006, pp. 585–611. — Detailed biomechanical analysis of plantar fasciitis development.
Methodology: Treatment recommendations in this article reflect current clinical consensus and are graded by the strength of supporting evidence. Conservative treatments are recommended as first-line interventions consistent with guidelines from the American College of Foot and Ankle Surgeons (ACFAS) and the American Physical Therapy Association (APTA). Product recommendations are based on clinical utility, patient feedback, and alignment with evidence-based treatment principles. This article is intended for informational purposes and does not constitute medical advice. Consult a qualified healthcare provider for diagnosis and personalized treatment.
Reviewed and updated: March 2026. For more guides on managing heel pain and related foot conditions, explore our full library at plantarfasciitisguides.com.
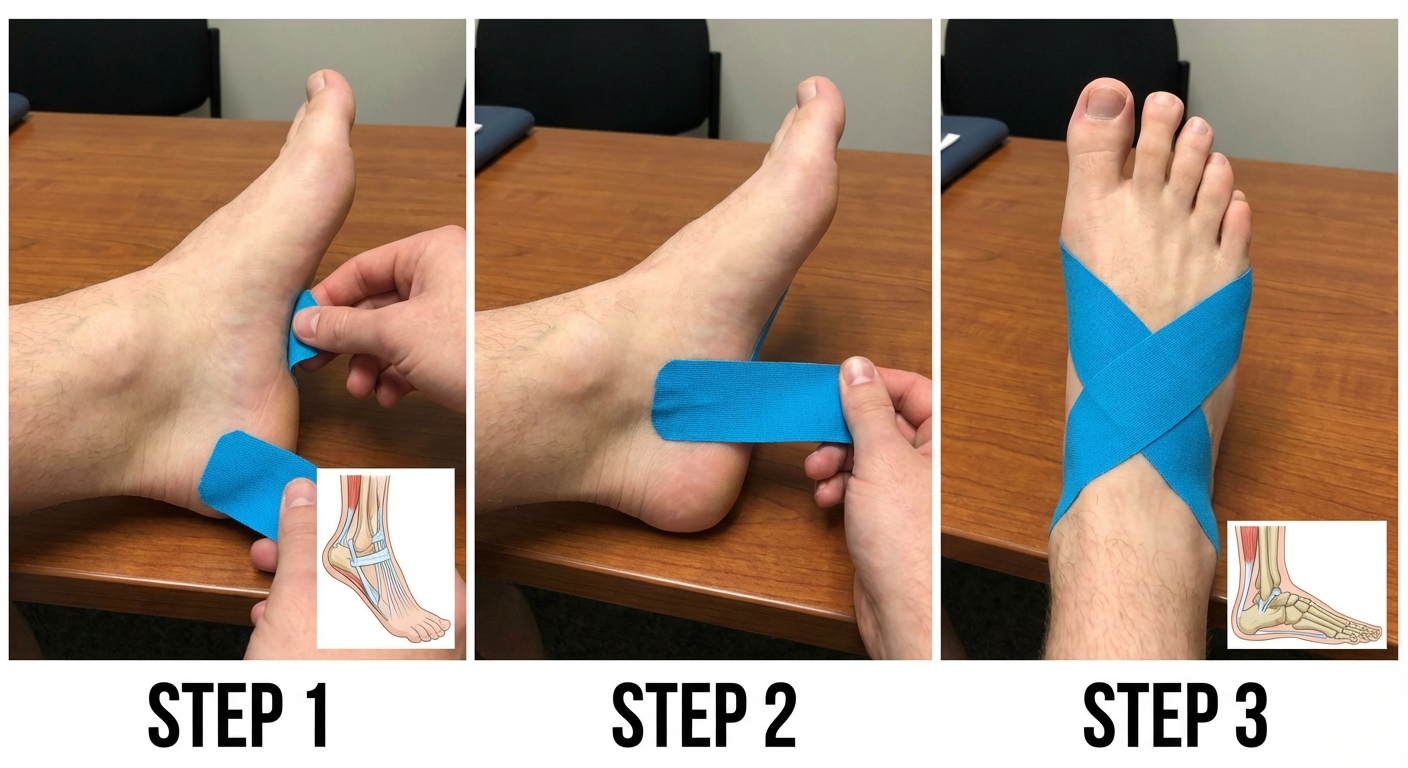 Kinesiology tape applied to the plantar fascia can reduce pain by 40-60% during activity
Kinesiology tape applied to the plantar fascia can reduce pain by 40-60% during activity