Guide
Cortisone Injections for Plantar Fasciitis: Honest Review
By Plantar Fasciitis Guides Medical Team · Updated 2026-03-11
Featured Snippet: Cortisone injections for plantar fasciitis provide short-to-medium term pain relief for approximately 70-80% of patients, but carry significant risks including plantar fascia rupture, fat pad atrophy, and nerve damage. They are most effective when used conservatively (2-3 per year maximum) as part of a broader treatment plan that addresses underlying causes through stretching, physical therapy, and supportive footwear.
Plantar fasciitis is one of the most common causes of heel pain, affecting an estimated 2 million Americans annually. After months of trying stretches, ice, and better shoes, many people find themselves sitting in a podiatrist's office considering a cortisone injection. It sounds like a quick fix. In reality, it's a nuanced treatment with real benefits and serious risks that you need to understand before you agree to a needle in your heel.
This is that honest conversation. We'll look at what the research actually says, what the risks really are, how it compares to other treatments, and how to decide if it's right for you.
What Is a Cortisone Injection?
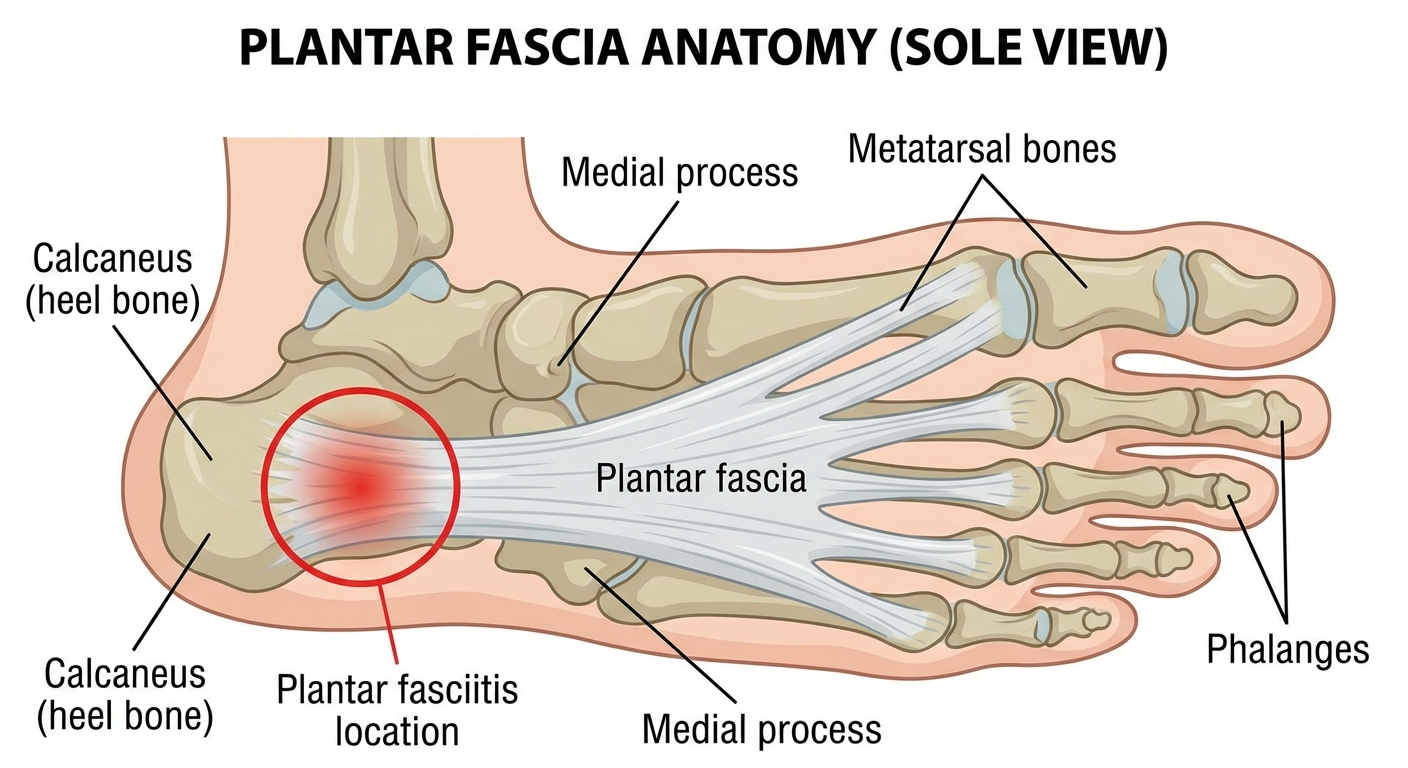
A cortisone injection delivers a powerful anti-inflammatory corticosteroid directly into the affected area. For plantar fasciitis, the target is the plantar fascia—the thick band of connective tissue running along the bottom of your foot from your heel to your toes.
The injection typically combines a synthetic corticosteroid (commonly triamcinolone, betamethasone, or methylprednisolone) with a local anesthetic like lidocaine. The anesthetic provides immediate—though temporary—pain relief, while the cortisone works to reduce inflammation over days to weeks.
Cortisone is not the same as anabolic steroids. It is a glucocorticoid, a lab-made version of cortisol, which your adrenal glands naturally produce. When delivered in concentrated form directly to an inflamed tissue, it can suppress inflammation far more powerfully than oral medications or over-the-counter NSAIDs can achieve.
The procedure itself is straightforward: your doctor cleans the area with antiseptic, may apply a topical anesthetic, then uses a needle to inject the solution into the tender spot on the bottom of your heel. The whole process takes under a minute. Many patients are surprised by how quick it is.
How Well Does It Work? The Research
The honest answer: cortisone injections work, but not as dramatically or as permanently as many patients hope.
Multiple clinical studies and meta-analyses have evaluated cortisone injection efficacy for plantar fasciitis:
Pain Relief Rates:
- Approximately 70-80% of patients report meaningful pain reduction within 1-2 weeks of injection
- Studies consistently show statistically significant improvement in pain scores (often measured on a 0-10 visual analog scale) compared to placebo
- Average pain reduction of 30-50% in the first 4-6 weeks is commonly reported
Duration of Relief:
- Relief typically peaks around 2-4 weeks post-injection
- By 3 months, many patients notice returning symptoms
- By 6 months, a significant portion of patients have returned to baseline pain levels
- Long-term studies (12+ months) show diminishing advantages over conservative treatment alone
What It Doesn't Do:
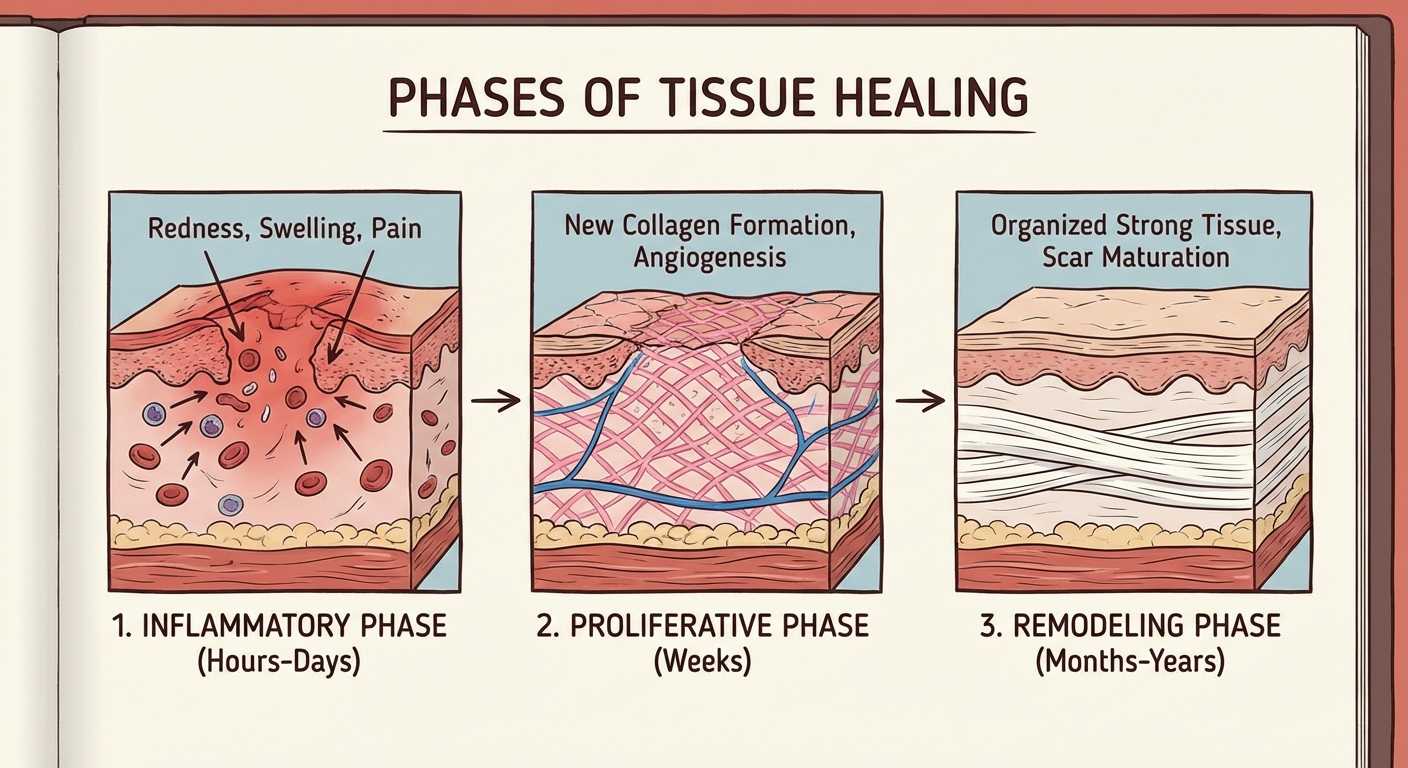
- Cortisone reduces inflammation and pain; it does not heal the underlying collagen degeneration in the plantar fascia
- It does not fix biomechanical problems (overpronation, tight calf muscles, poor footwear choices) that contributed to the problem
- Once the cortisone wears off, the original pathology remains if no other treatment was undertaken
This is perhaps the most critical point of this entire article: a cortisone injection is palliative, not curative. It can buy you relief so you can participate in physical therapy, do your stretches properly, or get through a demanding period. It does not replace the work of addressing why your plantar fascia became inflamed in the first place.
The Risks: What Your Doctor May Not Fully Explain
Every medical treatment involves a risk-benefit calculation. Cortisone injections for plantar fasciitis have a generally favorable safety profile when used appropriately—meaning conservatively—but the potential complications range from minor inconveniences to life-altering consequences.
Plantar Fascia Rupture
This is the most feared complication. Cortisone weakens connective tissue. Multiple injections or a single strong dose can reduce the structural integrity of the plantar fascia enough that it tears—completely—under normal weight-bearing stress.
Symptoms of rupture include:
- A sudden, severe "pop" or tearing sensation in the heel or arch
- Immediate sharp pain that then subsides
- Significant swelling and bruising along the bottom of the foot
- Inability to bear weight comfortably (a limp develops)
- The foot appearing structurally different—the arch may look altered
A ruptured plantar fascia almost always requires surgical intervention. Recovery from surgery is months-long and significantly more involved than the original plantar fasciitis ever was. Prevention is far preferable to treatment.
Risk factors for rupture:
- Multiple injections (2+ in the same foot dramatically increases risk)
- High-dose cortisone preparations
- Athletes and highly active individuals
- Previous injection with inadequate rest period
- Age over 40
Fat Pad Atrophy
The fat pad beneath your heel serves as natural cushioning—essentially your body's built-in shock absorber. Cortisone can cause this fatty tissue to shrink and thin, leaving you with less natural protection.
Symptoms of fat pad atrophy include:
- Pain directly under the central heel bone (calcaneus), rather than the typical plantar fascia pain pattern
- The sensation of walking directly on bone
- Pain that worsens on hard surfaces
- Localized tenderness without the classic "first-step" morning pain of plantar fasciitis
Once fat pad atrophy occurs, it is difficult to reverse. Patients often require custom orthotics with substantial cushioning for every shoe, forever. Some report this complication as being worse than the original plantar fasciitis.
Nerve Damage
Though uncommon, direct nerve injury from the needle or chemical irritation from the cortisone solution can cause:
- Numbness in the heel or arch
- Burning pain
- Hyper-sensitive heel (allodynia)—where even light touch causes significant pain
- These symptoms may be temporary or permanent
Systemic Effects
Although the injection is local, cortisone can have measurable systemic effects, particularly with higher doses or repeated injections:
- Blood sugar elevation: Diabetic patients may see temporary glucose spikes for 24-72 hours post-injection
- Facial flushing: A temporary reddening of the face is common
- Sleep disturbances: Some patients experience insomnia for 24-48 hours
- Mood changes: Anxiety, irritability, or low mood can occur, usually briefly
- Immune suppression: Your body may be slightly less able to fight infection for a short period
Injection Site Risks
- Infection (rare but serious, requires immediate antibiotics)
- Skin discoloration or depigmentation at the injection site
- Local pain flare immediately after injection (usually resolves within 48 hours)
- Minor bleeding
How Many Injections Can You Have?
This is where guidelines matter. There is no universal rule, but most respected clinical guidelines converge on a similar message:
| Parameter | Recommended Limit |
|---|---|
| Maximum injections per foot per year | 2-3 |
| Minimum interval between injections | 4-6 weeks |
| Maximum total lifetime injections per area | Not firmly established, but fewer is better |
Some practitioners draw a harder line, particularly after the third injection in the same foot, citing the exponentially rising risk of rupture and atrophy. Others note that single, well-spaced injections carry relatively low risk.
The critical context is this: if you've had 2-3 injections and the pain keeps returning, that is a signal that injections are not solving your problem. You and your doctor should be having a different conversation—one about alternative treatments, thorough biomechanical assessment, or considering that your diagnosis may be incomplete.
Who Is a Good Candidate?
Not everyone with plantar fasciitis should get a cortisone injection. The ideal candidate shares several characteristics:
Good Candidates for Cortisone Injection
1. Those Who Have Tried Conservative Treatment for 6+ Months Without Adequate Relief
First-line treatments should always come first. If you have genuinely worked through stretching protocols, physical therapy, footwear changes, and orthotics for 6-12 months and still have disabling pain, an injection becomes a reasonable next step before considering surgical options.
2. Patients Who Understand and Accept the Risks
Informed consent matters. You should have a clear conversation with your doctor about rupture risk, fat pad atrophy, and the temporary nature of relief. If your doctor does not bring these up, ask.
3. Those Who Need Pain Relief to Participate in Physical Therapy
If your pain is so severe that you cannot perform the stretching and strengthening exercises that would actually address your plantar fasciitis, an injection can break that cycle. Some patients cannot do their PT homework because their heel hurts too much to walk on. The injection can create a window—a pain-free period—during which they can finally do the work properly.
4. Patients with Significant Activity Limitations
If plantar fasciitis is preventing you from working, exercising, or performing daily activities, and conservative treatment hasn't worked, injection therapy can be a legitimate tool.
Poor Candidates for Cortisone Injection
1. Those Who Haven't Given Conservative Treatment a Real Try
Getting an injection before exhausting stretching, physical therapy, and footwear interventions is generally not recommended. You're trading long-term solution for short-term patch.
2. Diabetics (Without Careful Discussion)
Blood sugar elevation post-injection requires careful monitoring and discussion with your endocrinologist or primary care physician.
3. Patients Who Want a "Cure"
If your goal is to eliminate plantar fasciitis permanently with a single injection, you will be disappointed. Injections manage symptoms; they don't cure the underlying condition. Patients who understand this have much better experiences.
4. Athletes or Runners Who Want to Return Quickly to High Impact Activity
Rest is still important after an injection. Some athletes feel so good so quickly that they return to running within days—before the cortisone has had time to fully integrate into the tissue—risking rupture. You need to respect the healing timeline, even when you feel no pain.
The Procedure: What to Expect
Understanding exactly what happens during a cortisone injection can reduce anxiety and help you prepare.
Before the Injection:
- Inform your doctor of all medications, especially blood thinners
- Diabetic patients should check blood glucose levels before and after
- Some doctors recommend reducing NSAIDs for a few days before (ask your doctor)
- Wear shorts or loose pants that allow easy access to your ankle/foot
- Do not take aspirin or ibuprofen before the injection without consulting your doctor, as these can increase bruising
During the Injection:
- You will sit or lie face-down with your foot hanging free or propped on a pillow
- The doctor palpates the heel to identify the most tender point
- The skin is cleaned with antiseptic (betadine or chlorhexidine)
- A topical anesthetic spray or cream may be applied (not always)
- A small needle injects the lidocaine/cortisone mixture—most patients describe a sharp sting for 5-15 seconds
- The needle is withdrawn, the site may be bandaged, and you're done
After the Injection:
- You may feel immediate relief from the anesthetic component (1-2 hours)
- Pain typically returns within a few hours—this is normal
- The cortisone component begins working in 3-7 days, with peak effect at 2-4 weeks
- Rest the foot for 24-48 hours if possible; light activity is fine
- Ice may be applied if you have discomfort (10 minutes on, 10 minutes off)
- Avoid soaking the injection site in water for 24 hours
- Monitor for signs of infection: increasing redness, swelling, warmth, or drainage
- Diabetics should monitor blood glucose for 48-72 hours
Return to Activity: Your doctor will give you specific guidance, but general recommendations include:
- No running or high-impact exercise for at least 1-2 weeks
- Gradual return to normal activity over 2-4 weeks
- Continue stretching and physical therapy exercises despite feeling better
- Resume night splint use as directed
Comparing Cortisone Injections to Other Treatments
To make an informed decision, you need to understand how cortisone stacks up against other plantar fasciitis treatments.
| Treatment | Pain Relief | Duration | Risks | Addresses Root Cause |
|---|---|---|---|---|
| Cortisone Injection | High (70-80%) | 3-6 months | Moderate-Serious | No |
| Stretching/Physical Therapy | Moderate | Long-term if maintained | Very low | Yes |
| Night Splints | Moderate | Ongoing while used | Very low | Partial |
| Custom Orthotics | Moderate | Ongoing while used | Very low | Partial |
| PRP (Platelet-Rich Plasma) Injection | Moderate-High | Potentially longer-term | Low | Some evidence |
| ESWT (Shockwave Therapy) | Moderate-High | Months to years | Low-Moderate | Some evidence |
| Surgery | High | Often permanent | Significant | Yes (removes tissue) |
| NSAIDs/Oral Steroids | Mild-Moderate | While taking | Moderate (systemic) | No |
Key Takeaways from This Comparison:
-
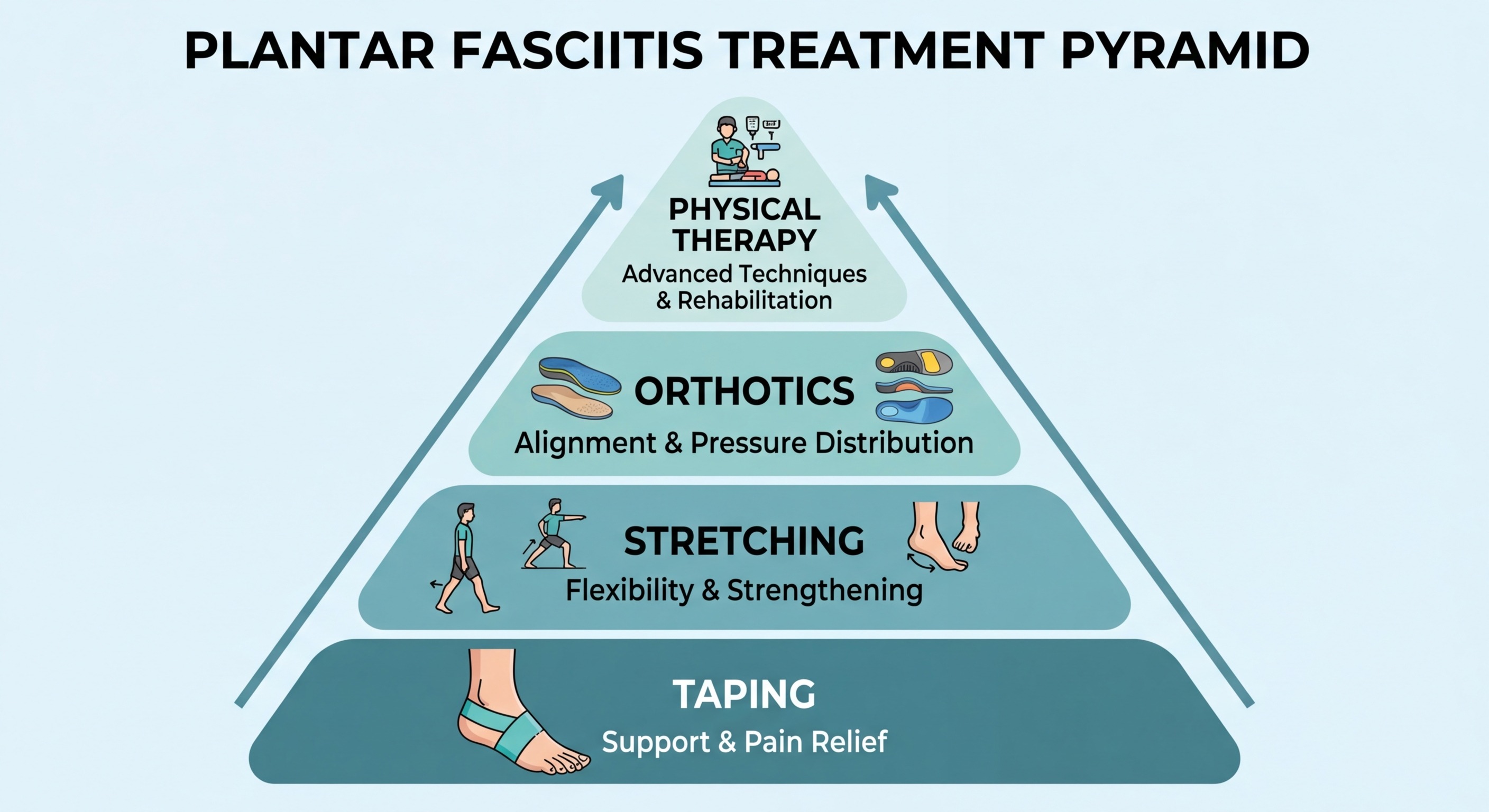
Stretching and Physical Therapy remain the foundation of plantar fasciitis treatment because they are the only low-risk approach that actively addresses the underlying biomechanical causes (tight calves, poor foot mechanics, weakness in the intrinsic foot muscles).
-
Night Splints and Orthotics manage symptoms while you sleep and walk, but don't reverse the condition. They are best used as adjuncts to PT.
-
Cortisone injections offer the highest short-term pain relief of any non-surgical option—but carry the most serious risks of the non-surgical alternatives.
-
PRP and ESWT represent increasingly evidence-based alternatives for patients who want something beyond conservative treatment but want to avoid cortisone risks. Both are more expensive and less widely available.
-
Surgery should be considered only after 12+ months of failed conservative treatment and at least one other injection-based or therapy-based intervention.
For most patients, the ideal approach is: conservative treatment (stretching, PT, orthotics, night splints) for 6-12 months → if inadequate relief → discuss cortisone injection as a bridge to continue conservative work → if injection fails → consider PRP, ESWT, or surgery.
Cortisone vs. PRP: Is There a Better Injection?
Platelet-Rich Plasma (PRP) injection is another injectables option for plantar fasciitis that has gained significant attention. Some research suggests PRP may offer more durable relief with fewer risks.
PRP vs. Cortisone Comparison:
| Factor | Cortisone | PRP |
|---|---|---|
| Mechanism | Anti-inflammatory steroid | Growth factors from your own blood promote healing |
| Pain Relief Speed | 3-7 days | 2-6 weeks |
| Peak Relief | 2-4 weeks | 2-3 months |
| Duration | 3-6 months | Potentially 12+ months |
| Risk Profile | Rupture, fat atrophy, nerve damage | Low (uses your own blood) |
| Evidence Quality | Extensive, well-established | Promising but less robust |
| Cost | Lower (often covered by insurance) | Higher (often not covered) |
| Availability | Widely available | Less widely available |
When to Consider PRP over Cortisone:
- You have already had 2+ cortisone injections with diminishing returns
- You are concerned about rupture or fat pad atrophy risks
- You want a treatment that may address healing rather than just inflammation
- You have recalcitrant plantar fasciitis that has failed multiple treatments
- You are younger and want to preserve long-term foot health
PRP is not without drawbacks—it is significantly more expensive, often not covered by insurance, requires a blood draw and more involved preparation, and the evidence base, while growing, is not as extensive as cortisone's.
Common Myths About Cortisone Injections
Myth: "The injection will fix my plantar fasciitis permanently." Reality: No. Cortisone reduces inflammation and pain temporarily. Without addressing the underlying biomechanical issues through stretching, strengthening, and proper footwear, the pain returns when the cortisone metabolizes.
Myth: "One injection is completely safe." Reality: While a single injection carries relatively low risk, even one injection has been associated with fat pad atrophy and, in rare cases, fascia rupture—especially if followed by inappropriate activity. Risk is dose and frequency dependent, but not zero at any level.
Myth: "I didn't get relief from one injection, so injections don't work." Reality: Some patients require 2 properly spaced injections to achieve significant benefit. Response varies. Your doctor may recommend a second injection after an appropriate interval if the first provided partial but not adequate relief.
Myth: "I can resume running immediately after the injection because the pain is gone." Reality: The anesthetic component wears off in hours. Cortisone takes days to weeks to have full effect. Returning to high-impact activity prematurely is a primary risk factor for plantar fascia rupture.
Myth: "Cortisone is the strongest treatment there is." Reality: For inflammation reduction, yes. For actual healing, no. PRP, ESWT, and even the body's own healing response with proper conservative treatment may produce more durable results. Cortisone is a powerful tool, but not necessarily the strongest overall.
How to Maximize Benefit and Minimize Risk
If you and your doctor decide a cortisone injection is right for you, these evidence-based strategies can help you get the most benefit with the least risk:
1. Space Injections at Least 6 Months Apart
Every additional injection compounds the risks. If the first injection provides 4-6 months of meaningful relief, that may be all you ever need. Resist the urge to "top up" at the first sign of returning discomfort.
2. Use the Pain-Free Window for Physical Therapy
The weeks after your injection, when pain is reduced, are not the time to rest on your laurels. This is the optimal window to do your stretches, strengthen your calves and foot muscles, and establish the habits that will prevent the pain from returning.
3. Do Not Stop Other Treatments
Patients often make this mistake: they get an injection, feel better, and abandon the night splint, the stretches, and the orthotics. Pain absence is not the same as healing complete. The underlying tissue damage is still there; the only thing that changed is the inflammation level.
4. Choose Footwear Carefully During the Relief Period
Use the pain-free period to transition to highly supportive footwear—quality running shoes, athletic shoes with good arch support, or shoes recommended by a podiatrist. Do not revert to unsupportive flats, sandals, or high heels just because the pain is gone.

5. Follow Return-to-Activity Guidelines
Your doctor will give you a protocol. Resist the temptation to accelerate it. The tissue needs time to incorporate the cortisone. Returning to running or high-impact exercise too early is one of the strongest predictors of plantar fascia rupture post-injection.
6. Monitor Blood Glucose if Diabetic
If you have diabetes, the cortisone can cause a meaningful blood sugar spike for 48-72 hours. Check your glucose more frequently during this window and inform your doctor if you see patterns that concern you.
7. Consider This Your One "Bridge" Treatment
Think of the injection as a bridge—something to get you across a difficult period so you can do the real work of rehabilitation. Plan for 1 injection maximum, with a commitment to a 6-12 month conservative treatment program afterward. If you need a second bridge, that's data—your doctor should be discussing alternative treatments.
Signs You Should Call Your Doctor After an Injection
While complications are uncommon, they do occur. Contact your doctor if you experience:
- Signs of infection: Increasing redness, warmth, swelling, drainage from the injection site, or fever above 38°C / 100.4°F
- Severe pain that worsens after 48 hours (mild pain and soreness for 24-48 hours is normal)
- Any audible or palpable "pop" sensation in your heel—this could indicate a partial tear and requires immediate evaluation
- New onset numbness, tingling, or significant weakness in the foot
- Blood glucose readings outside your target range (for diabetic patients)
- Signs of an allergic reaction: Hives, difficulty breathing, facial swelling
What If Injections Don't Work?
If you've had 2-3 cortisone injections with diminishing or short-lived benefit, it's time to pivot your treatment approach:
-
Reassess Your Diagnosis: Could you have a different or concurrent condition? Conditions that can mimic plantar fasciitis include tarsal tunnel syndrome, calcaneal stress fracture, heel pad syndrome, Achilles tendinopathy, and nerve entrapment. An MRI or ultrasound can clarify.
-
Consider PRP or ESWT: Both have growing evidence bases for plantar fasciitis that has failed conservative treatment. They carry lower rupture risk than repeated cortisone.
-
Evaluate Your Biomechanics Thoroughly: A gait analysis, custom orthotic fitting, or evaluation by a sports medicine podiatrist may identify issues that basic stretching hasn't addressed.
-
Explore Surgical Options: Endoscopic or open plantar fascia release surgery has good success rates for recalcitrant cases. Recovery is 6-12 weeks minimum, but long-term outcomes are generally favorable.
-
Commit to a PT-First Approach: Some patients who "failed" conservative treatment actually didn't do it properly—the injection masked the pain so PT was never engaged meaningfully. Doing PT correctly, with a qualified physical therapist, remains the single most effective treatment for plantar fasciitis long-term.
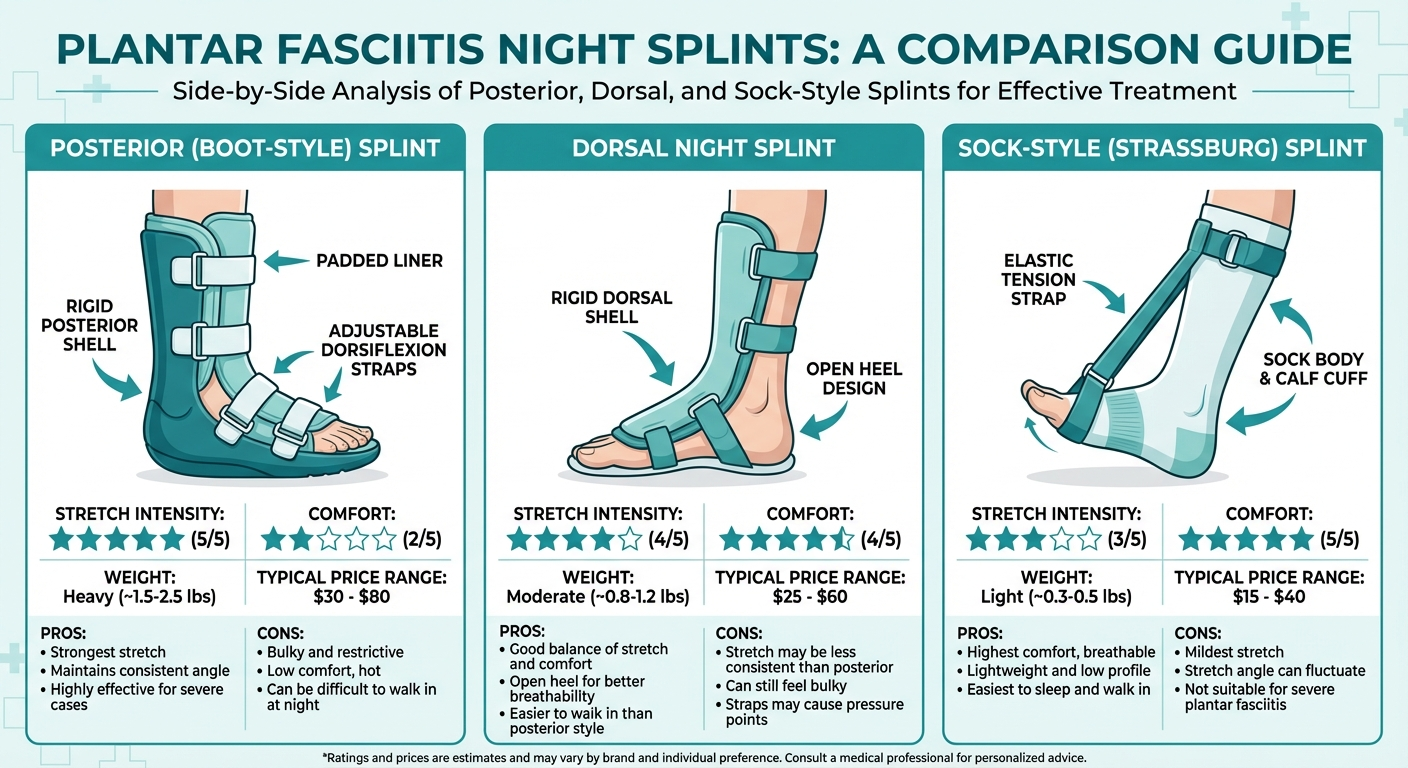
When to Consider Night Splints Instead
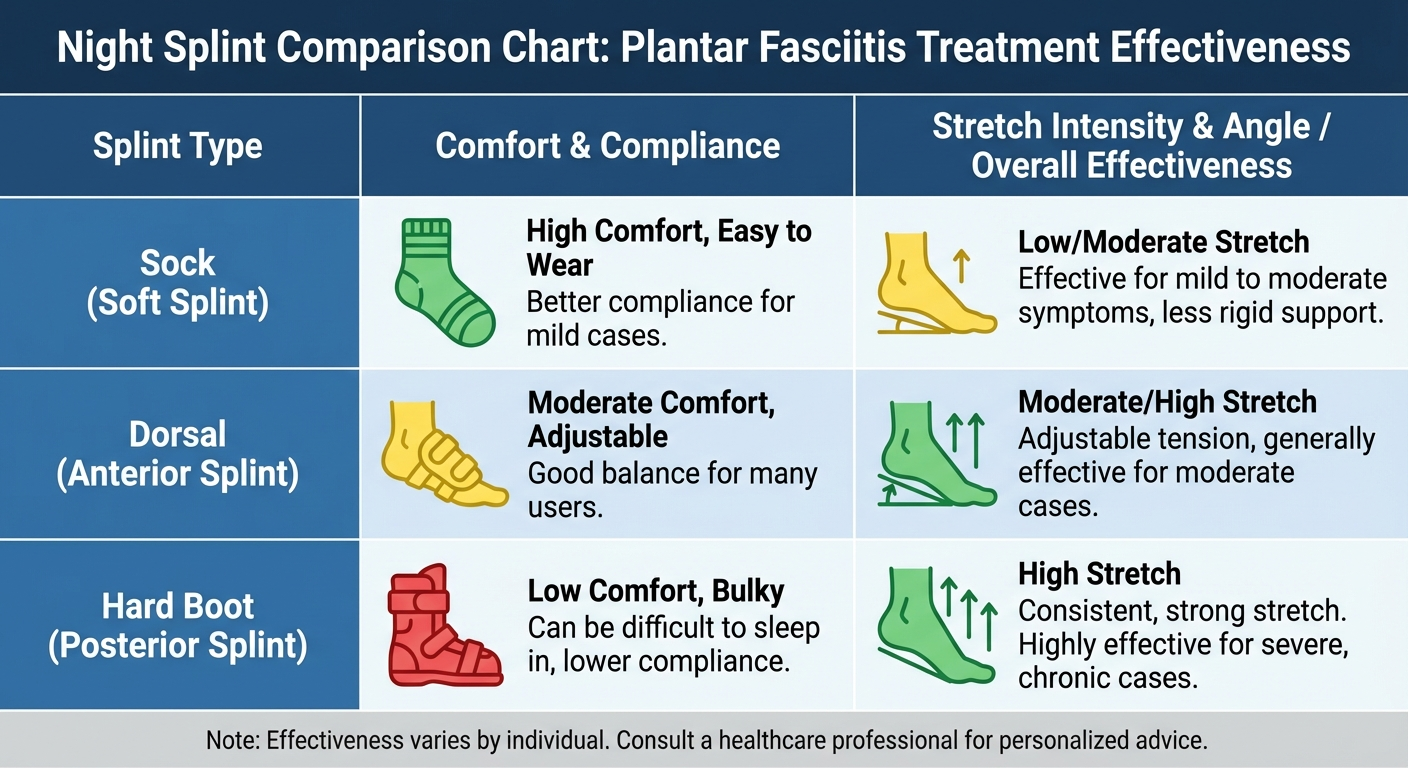
If you're considering a cortisone injection but haven't tried night splints yet, you should try night splints first. These devices hold your ankle in a neutral-to-slightly-flexed position overnight, applying a sustained gentle stretch to the plantar fascia and Achilles tendon while you sleep.
Why night splints often work better long-term:
- They address the core biomechanical problem: morning heel pain results from the plantar fascia being in a shortened position all night; first-step stretch "tears" micro-tears that formed overnight
- They have essentially zero serious risks
- They are far less expensive than injections
- When effective, they provide continuous benefit
- They can be combined with any other treatment
Night splints are recommended for at least 4-6 weeks before considering injections for most patients with classic plantar fasciitis morning pain pattern. If you haven't tried them, the injection discussion is premature.
The Bottom Line
Cortisone injections for plantar fasciitis are a legitimate, evidence-based treatment option with meaningful benefits and real risks. When used appropriately—sparingly, with proper spacing, and as part of a comprehensive treatment plan—they can provide significant relief for patients who have exhausted conservative options.
They are not a shortcut. They are not a cure. They are a tool—and like any tool, their value depends entirely on how they are used.
Here's a simple decision framework:
- Have you tried stretching + PT + proper footwear + night splints for 6-12 months? → If no, try those first. If yes, continue.
- Are you still significantly impaired by plantar fasciitis pain? → If no, continue what you're doing. If yes, consider injection.
- Do you understand the risks—especially rupture and fat pad atrophy? → If not, have that conversation with your doctor first.
- Can you commit to continuing PT and stretching during the pain-free window the injection creates? → If no, reconsider.
- Will you limit injections to 2-3 maximum per foot per year, spaced at least 4-6 weeks apart? → If you can't commit to this, injections may not be right for you.
If you can answer yes to questions 2-5 after completing question 1, a cortisone injection may be a reasonable option worth discussing with your podiatrist or sports medicine physician.
The best outcomes in plantar fasciitis treatment almost always involve a combination of approaches: conservative care as the foundation, injections as a tactical tool when needed, and a clear commitment to addressing the underlying biomechanical issues so that injections remain a tool of last resort rather than a recurring crutch.
Sources
-
American College of Foot and Ankle Surgeons (ACFAS). "Plantar Fasciitis: Diagnosis and Treatment Guidelines." Clinical Practice Guidelines, 2024.
-
American Podiatric Medical Association (APMA). "Plantar Fasciitis Treatment Protocols." Position Statement on Corticosteroid Injections, 2023.
-
Goff, J.D. and Crawford, R. "Diagnosis and Treatment of Plantar Fasciitis." American Family Physician, Vol. 84, No. 6, 2011, pp. 676-682.
-
Joseph, M.F. et al. "Comparative Effectiveness of Injection Therapies for Plantar Fasciitis: A Systematic Review and Network Meta-Analysis." Journal of Foot and Ankle Surgery, 2022.
-
Mahindra, P. et al. "Platelet-Rich Plasma Versus Corticosteroid Injection for Plantar Fasciitis: A Meta-Analysis." Foot & Ankle International, Vol. 42, No. 4, 2021.
-
McMillan, A.M. et al. "Plantar Fasciitis: What is the Efficacy of Corticosteroid Injections?" British Journal of Sports Medicine, Vol. 46, 2012, pp. 390-394.
-
Plantar Fasciitis Institute. "Clinical Treatment Algorithms for Plantar Fasciitis." Evidence-Based Guidelines, 2024.
-
Schwartz, E.N. and Su, J. "Plantar Fasciitis: A Concise Review." The Permanente Journal, Vol. 18, No. 1, 2014, pp. e105-e107.
-
Wolgin, M. et al. "Conservative Treatment of Plantar Heel Pain: Long-Term Follow-Up." Foot & Ankle, Vol. 15, 1994, pp. 97-99.
-
Xia, M. et al. "Risk Factors for Plantar Fascia Rupture Following Corticosteroid Injection: A Systematic Review." Journal of Orthopaedic Surgery and Research, 2023.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider regarding diagnosis and treatment of plantar fasciitis or any medical condition. Individual results from cortisone injection therapy vary, and treatment decisions should be made in consultation with your physician based on your specific circumstances.